{"title":"梅克尔憩室伴中憩室带引起大面积肠坏疽--病例报告","authors":"Basil Babu, Satish Subbiah Nagaraj, Swastika Sharma","doi":"10.1007/s42399-024-01650-0","DOIUrl":null,"url":null,"abstract":"<p>Meckel’s diverticulum is the most common congenital anomaly of the gastrointestinal tract. The anatomy of Meckel’s diverticulum varies, and when it is attached to the abdominal wall or mesentery by means of fibrous cords, it can cause obstruction including massive bowel gangrene which has not yet been reported in the literature. A middle-aged man presented to the emergency wing with a history of obstipation and vomiting for 2 days. A CECT (Contrast Enhanced Computed Tomography) abdomen revealed dilated ileal bowel loops with multiple strictures, mesenteric lymph nodes, and mild ascites. With a provisional diagnosis of tuberculosis of the abdomen, he was taken for emergency laparotomy. Around 200 cm of distal ileum was found gangrenous due to the herniation of it beneath a mesodiverticular band which was connected to the apex of Meckel’s diverticulum found 50 cm from the ileocolic junction. The gangrenous bowel along with the gangrenous Meckel’s diverticulum was resected, and an end ileostomy and distal mucosal fistula were made. Meckel’s diverticulum must be kept as a differential in any young patients presenting with acute intestinal obstruction with no previous history of abdominal surgery, TB abdomen, or inflammatory bowel disease. While recommendations suggest resection of symptomatic Meckel’s diverticulum with a narrow base and wide body due to its propensity to rotate along its axis and cause gangrene of Meckel’s diverticulum, we believe Meckel’s diverticulum with a band attaching it to umbilicus or with ileal mesentery must be considered for resection to prevent grave complications.</p>","PeriodicalId":21944,"journal":{"name":"SN Comprehensive Clinical Medicine","volume":"8 1","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2024-02-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Meckel’s Diverticulum with a Mesodiverticular Band Causing Massive Bowel Gangrene—A Case Report\",\"authors\":\"Basil Babu, Satish Subbiah Nagaraj, Swastika Sharma\",\"doi\":\"10.1007/s42399-024-01650-0\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Meckel’s diverticulum is the most common congenital anomaly of the gastrointestinal tract. The anatomy of Meckel’s diverticulum varies, and when it is attached to the abdominal wall or mesentery by means of fibrous cords, it can cause obstruction including massive bowel gangrene which has not yet been reported in the literature. A middle-aged man presented to the emergency wing with a history of obstipation and vomiting for 2 days. A CECT (Contrast Enhanced Computed Tomography) abdomen revealed dilated ileal bowel loops with multiple strictures, mesenteric lymph nodes, and mild ascites. With a provisional diagnosis of tuberculosis of the abdomen, he was taken for emergency laparotomy. Around 200 cm of distal ileum was found gangrenous due to the herniation of it beneath a mesodiverticular band which was connected to the apex of Meckel’s diverticulum found 50 cm from the ileocolic junction. The gangrenous bowel along with the gangrenous Meckel’s diverticulum was resected, and an end ileostomy and distal mucosal fistula were made. Meckel’s diverticulum must be kept as a differential in any young patients presenting with acute intestinal obstruction with no previous history of abdominal surgery, TB abdomen, or inflammatory bowel disease. While recommendations suggest resection of symptomatic Meckel’s diverticulum with a narrow base and wide body due to its propensity to rotate along its axis and cause gangrene of Meckel’s diverticulum, we believe Meckel’s diverticulum with a band attaching it to umbilicus or with ileal mesentery must be considered for resection to prevent grave complications.</p>\",\"PeriodicalId\":21944,\"journal\":{\"name\":\"SN Comprehensive Clinical Medicine\",\"volume\":\"8 1\",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-02-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"SN Comprehensive Clinical Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s42399-024-01650-0\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"SN Comprehensive Clinical Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s42399-024-01650-0","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Meckel’s Diverticulum with a Mesodiverticular Band Causing Massive Bowel Gangrene—A Case Report
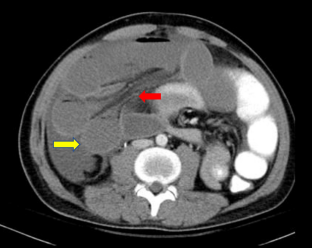
Meckel’s diverticulum is the most common congenital anomaly of the gastrointestinal tract. The anatomy of Meckel’s diverticulum varies, and when it is attached to the abdominal wall or mesentery by means of fibrous cords, it can cause obstruction including massive bowel gangrene which has not yet been reported in the literature. A middle-aged man presented to the emergency wing with a history of obstipation and vomiting for 2 days. A CECT (Contrast Enhanced Computed Tomography) abdomen revealed dilated ileal bowel loops with multiple strictures, mesenteric lymph nodes, and mild ascites. With a provisional diagnosis of tuberculosis of the abdomen, he was taken for emergency laparotomy. Around 200 cm of distal ileum was found gangrenous due to the herniation of it beneath a mesodiverticular band which was connected to the apex of Meckel’s diverticulum found 50 cm from the ileocolic junction. The gangrenous bowel along with the gangrenous Meckel’s diverticulum was resected, and an end ileostomy and distal mucosal fistula were made. Meckel’s diverticulum must be kept as a differential in any young patients presenting with acute intestinal obstruction with no previous history of abdominal surgery, TB abdomen, or inflammatory bowel disease. While recommendations suggest resection of symptomatic Meckel’s diverticulum with a narrow base and wide body due to its propensity to rotate along its axis and cause gangrene of Meckel’s diverticulum, we believe Meckel’s diverticulum with a band attaching it to umbilicus or with ileal mesentery must be considered for resection to prevent grave complications.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


