Daniel de Luis Román, Juana Carretero Gómez, José Manuel García-Almeida, Fernando Garrachón Vallo, German Guzmán Rolo, Juan José López Gómez, Francisco José Tarazona-Santabalbina, Alejandro Sanz-Paris
{"title":"糖尿病性肌肉疏松症。糖尿病患者肌肉筛查方案建议","authors":"Daniel de Luis Román, Juana Carretero Gómez, José Manuel García-Almeida, Fernando Garrachón Vallo, German Guzmán Rolo, Juan José López Gómez, Francisco José Tarazona-Santabalbina, Alejandro Sanz-Paris","doi":"10.1007/s11154-023-09871-9","DOIUrl":null,"url":null,"abstract":"<h3 data-test=\"abstract-sub-heading\">Objectives</h3><p>To propose the grounds for “diabetic sarcopenia” as a new comorbidity of diabetes, and to establish a muscle screening algorithm proposal to facilitate its diagnosis and staging in clinical practice. Method: A qualitative expert opinion study was carried out using the nominal technique. A literature search was performed with the terms “screening” or “diagnostic criteria” and “muscle loss” or “sarcopenia” and “diabetes” that was sent to a multidisciplinary group of 7 experts who, in a face-to-face meeting, discussed various aspects of the screening algorithm. Results: The hallmark of diabetic sarcopenia (DS) is muscle mass atrophy characteristic of people with diabetes mellitus (DM) in contrast to the histological and physiological normality of muscle mass. The target population to be screened was defined as patients with DM with a SARC-F questionnaire > 4, glycosylated haemoglobin (HbA1C) ≥ 8.0%, more than 5 years since onset of DM, taking sulfonylureas, glinides and sodium/glucose cotransporter inhibitors (SGLT2), as well as presence of chronic complications of diabetes or clinical suspicion of sarcopenia. Diagnosis was based on the presence of criteria of low muscle strength (probable sarcopenia) and low muscle mass (confirmed sarcopenia) using methods available in any clinical consultation room, such as dynamometry, the chair stand test, and Body Mass Index (BMI)-adjusted calf circumference. DS was classified into 4 stages: Stage I corresponds to sarcopenic patients with no other diabetes complication, and Stage II corresponds to patients with some type of involvement. Within Stage II are three sublevels (a, b and c). Stage IIa refers to individuals with sarcopenic diabetes and some diabetes-specific impairment, IIb to sarcopenia with functional impairment, and IIc to sarcopenia with diabetes complications and changes in function measured using standard tests Conclusion: Diabetic sarcopenia has a significant impact on function and quality of life in people with type 2 diabetes mellitus (T2DM), and it is important to give it the same attention as all other traditionally described complications of T2DM. This document aims to establish the foundation for protocolising the screening and diagnosis of diabetic sarcopenia in a manner that is simple and accessible for all levels of healthcare.</p>","PeriodicalId":21105,"journal":{"name":"Reviews in Endocrine and Metabolic Disorders","volume":"167 1","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2024-02-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Diabetic Sarcopenia. A proposed muscle screening protocol in people with diabetes\",\"authors\":\"Daniel de Luis Román, Juana Carretero Gómez, José Manuel García-Almeida, Fernando Garrachón Vallo, German Guzmán Rolo, Juan José López Gómez, Francisco José Tarazona-Santabalbina, Alejandro Sanz-Paris\",\"doi\":\"10.1007/s11154-023-09871-9\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<h3 data-test=\\\"abstract-sub-heading\\\">Objectives</h3><p>To propose the grounds for “diabetic sarcopenia” as a new comorbidity of diabetes, and to establish a muscle screening algorithm proposal to facilitate its diagnosis and staging in clinical practice. Method: A qualitative expert opinion study was carried out using the nominal technique. A literature search was performed with the terms “screening” or “diagnostic criteria” and “muscle loss” or “sarcopenia” and “diabetes” that was sent to a multidisciplinary group of 7 experts who, in a face-to-face meeting, discussed various aspects of the screening algorithm. Results: The hallmark of diabetic sarcopenia (DS) is muscle mass atrophy characteristic of people with diabetes mellitus (DM) in contrast to the histological and physiological normality of muscle mass. The target population to be screened was defined as patients with DM with a SARC-F questionnaire > 4, glycosylated haemoglobin (HbA1C) ≥ 8.0%, more than 5 years since onset of DM, taking sulfonylureas, glinides and sodium/glucose cotransporter inhibitors (SGLT2), as well as presence of chronic complications of diabetes or clinical suspicion of sarcopenia. Diagnosis was based on the presence of criteria of low muscle strength (probable sarcopenia) and low muscle mass (confirmed sarcopenia) using methods available in any clinical consultation room, such as dynamometry, the chair stand test, and Body Mass Index (BMI)-adjusted calf circumference. DS was classified into 4 stages: Stage I corresponds to sarcopenic patients with no other diabetes complication, and Stage II corresponds to patients with some type of involvement. Within Stage II are three sublevels (a, b and c). Stage IIa refers to individuals with sarcopenic diabetes and some diabetes-specific impairment, IIb to sarcopenia with functional impairment, and IIc to sarcopenia with diabetes complications and changes in function measured using standard tests Conclusion: Diabetic sarcopenia has a significant impact on function and quality of life in people with type 2 diabetes mellitus (T2DM), and it is important to give it the same attention as all other traditionally described complications of T2DM. This document aims to establish the foundation for protocolising the screening and diagnosis of diabetic sarcopenia in a manner that is simple and accessible for all levels of healthcare.</p>\",\"PeriodicalId\":21105,\"journal\":{\"name\":\"Reviews in Endocrine and Metabolic Disorders\",\"volume\":\"167 1\",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-02-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Reviews in Endocrine and Metabolic Disorders\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s11154-023-09871-9\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Reviews in Endocrine and Metabolic Disorders","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s11154-023-09871-9","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
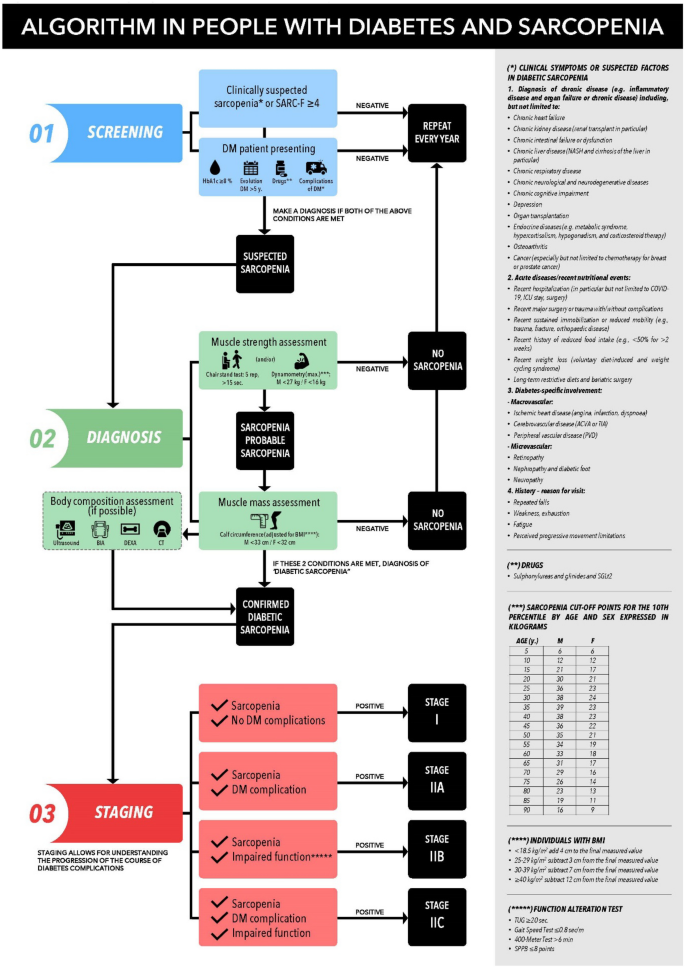
Diabetic Sarcopenia. A proposed muscle screening protocol in people with diabetes
Objectives
To propose the grounds for “diabetic sarcopenia” as a new comorbidity of diabetes, and to establish a muscle screening algorithm proposal to facilitate its diagnosis and staging in clinical practice. Method: A qualitative expert opinion study was carried out using the nominal technique. A literature search was performed with the terms “screening” or “diagnostic criteria” and “muscle loss” or “sarcopenia” and “diabetes” that was sent to a multidisciplinary group of 7 experts who, in a face-to-face meeting, discussed various aspects of the screening algorithm. Results: The hallmark of diabetic sarcopenia (DS) is muscle mass atrophy characteristic of people with diabetes mellitus (DM) in contrast to the histological and physiological normality of muscle mass. The target population to be screened was defined as patients with DM with a SARC-F questionnaire > 4, glycosylated haemoglobin (HbA1C) ≥ 8.0%, more than 5 years since onset of DM, taking sulfonylureas, glinides and sodium/glucose cotransporter inhibitors (SGLT2), as well as presence of chronic complications of diabetes or clinical suspicion of sarcopenia. Diagnosis was based on the presence of criteria of low muscle strength (probable sarcopenia) and low muscle mass (confirmed sarcopenia) using methods available in any clinical consultation room, such as dynamometry, the chair stand test, and Body Mass Index (BMI)-adjusted calf circumference. DS was classified into 4 stages: Stage I corresponds to sarcopenic patients with no other diabetes complication, and Stage II corresponds to patients with some type of involvement. Within Stage II are three sublevels (a, b and c). Stage IIa refers to individuals with sarcopenic diabetes and some diabetes-specific impairment, IIb to sarcopenia with functional impairment, and IIc to sarcopenia with diabetes complications and changes in function measured using standard tests Conclusion: Diabetic sarcopenia has a significant impact on function and quality of life in people with type 2 diabetes mellitus (T2DM), and it is important to give it the same attention as all other traditionally described complications of T2DM. This document aims to establish the foundation for protocolising the screening and diagnosis of diabetic sarcopenia in a manner that is simple and accessible for all levels of healthcare.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


