{"title":"利桑珠单抗对银屑病关节炎患者的疗效和安全性:随机对照试验的系统回顾和元分析","authors":"Qin-Yi Su, Hao-Nan Zhou, Guo-Mei Xia, Rui-Yuan Zhang, Hong-Yuan Tian, Chang Su, Yu-Xin Liu, He-Yi Zhang, Ting Cheng, Yue-Hong Huo, Qian Li, Sheng-Xiao Zhang","doi":"10.1007/s40744-024-00638-5","DOIUrl":null,"url":null,"abstract":"<h3 data-test=\"abstract-sub-heading\">Introduction</h3><p>Currently, the cause of psoriatic arthritis (PsA) is unknown, and the effectiveness of current drug treatments is unsatisfactory. In March 2019, the US Food and Drug Administration (FDA) approved risankizumab, a humanized immunoglobulin G1 (IgG1) monoclonal antibody targeting the p19 subunit of interleukin (IL)-23, for the treatment of PsA in adults. This study aimed to conduct a meta-analysis of double-blind, randomized, placebo-controlled trials to evaluate the effectiveness and safety of risankizumab in moderate-to-severe PsA.</p><h3 data-test=\"abstract-sub-heading\">Methods</h3><p>We conducted a thorough search of relevant databases from the establishment of the databases to October 1, 2023. We conducted a meta-analysis using Stata 12.0 and utilized <i>I</i><sup>2</sup> and Egger tests to assess heterogeneity and publication bias among the studies. Bias assessment was performed using the risk bias map and bias risk summary diagram generated by Revman5.4 software. The review protocols were registered on PROSPERO (CRD42023451894) and adhered to the preferred reporting item of system evaluation (PRISMA) guideline.</p><h3 data-test=\"abstract-sub-heading\">Results</h3><p>Six randomized controlled trials (RCTs) involving 5038 patients with PsA treated with either risankizumab or placebo were included in the analysis. At 24 weeks, the risankizumab group demonstrated a significantly higher American College of Rheumatology-20 (ACR20) response rate compared to the placebo group (RR 1.760, 95% CI 1.568–1.977, <i>P</i> < 0.001). Additionally, the risankizumab group showed a significantly higher Minimal Disease Activity (MDA) response rate compared to the placebo group (RR 1.827, 95% CI 1.048–3.184, <i>P</i> < 0.05). The risankizumab group also exhibited improvement in Short Form 36 Questionnaire (SF-36) score (SMD 0.51, 95% CI 0.33–0.69, <i>P</i> < 0.001), with significantly lower Health Assessment Questionnaire Disability Index (HAQ-DI) score (SMD − 0.27, 95% CI − 0.37 to − 0.17, <i>P</i> < 0.001) and higher Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) score (SMD 0.27, 95% CI 0.20–0.35, <i>P</i> < 0.001) compared to the placebo group. Moreover, the risankizumab group had a significantly lower Psoriasis Area and Severity Index (PASI) score (SMD − 6.12, 95% CI − 10.02 to 2.23, <i>P</i> < 0.001). A study by Mease et al. indicated that patients receiving risankizumab generally demonstrated numerical improvements in the Leeds Enthesitis Index (LEI), although the small sample size limits the evidence. Further research is necessary to provide evidence-based guidelines. There were no significant differences in the incidence of serious adverse events (SAE) and serious treatment-emergent adverse events (STEAE) between the risankizumab and placebo groups (RR 0.76, 95% CI 0.45–1.28, <i>P</i> = 0.31; RR 0.99, 95% CI 0.49–1.99, <i>P</i> = 0.97, respectively), and the overall incidence of adverse events (AE) was not comparable (RR 1.10, 95% CI 0.63–1.94, <i>P</i> = 0.73).</p><h3 data-test=\"abstract-sub-heading\">Conclusion</h3><p>Risankizumab showed superior efficacy across multiple outcome measures compared to placebo, with no significant increase in adverse events. Our findings endorse risankizumab as an excellent treatment option for PsA, offering valuable insights for clinicians and patients when choosing appropriate therapeutic interventions.</p><h3 data-test=\"abstract-sub-heading\">Trial Registration</h3><p>Retrospectively registered (CRD42023451894, 16 August 2023).</p>","PeriodicalId":21267,"journal":{"name":"Rheumatology and Therapy","volume":"46 1","pages":""},"PeriodicalIF":2.9000,"publicationDate":"2024-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Efficacy and Safety of Risankizumab in Patients with Psoriatic Arthritis: A Systematic Review and Meta-Analysis of Randomized Controlled Trials\",\"authors\":\"Qin-Yi Su, Hao-Nan Zhou, Guo-Mei Xia, Rui-Yuan Zhang, Hong-Yuan Tian, Chang Su, Yu-Xin Liu, He-Yi Zhang, Ting Cheng, Yue-Hong Huo, Qian Li, Sheng-Xiao Zhang\",\"doi\":\"10.1007/s40744-024-00638-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<h3 data-test=\\\"abstract-sub-heading\\\">Introduction</h3><p>Currently, the cause of psoriatic arthritis (PsA) is unknown, and the effectiveness of current drug treatments is unsatisfactory. In March 2019, the US Food and Drug Administration (FDA) approved risankizumab, a humanized immunoglobulin G1 (IgG1) monoclonal antibody targeting the p19 subunit of interleukin (IL)-23, for the treatment of PsA in adults. This study aimed to conduct a meta-analysis of double-blind, randomized, placebo-controlled trials to evaluate the effectiveness and safety of risankizumab in moderate-to-severe PsA.</p><h3 data-test=\\\"abstract-sub-heading\\\">Methods</h3><p>We conducted a thorough search of relevant databases from the establishment of the databases to October 1, 2023. We conducted a meta-analysis using Stata 12.0 and utilized <i>I</i><sup>2</sup> and Egger tests to assess heterogeneity and publication bias among the studies. Bias assessment was performed using the risk bias map and bias risk summary diagram generated by Revman5.4 software. The review protocols were registered on PROSPERO (CRD42023451894) and adhered to the preferred reporting item of system evaluation (PRISMA) guideline.</p><h3 data-test=\\\"abstract-sub-heading\\\">Results</h3><p>Six randomized controlled trials (RCTs) involving 5038 patients with PsA treated with either risankizumab or placebo were included in the analysis. At 24 weeks, the risankizumab group demonstrated a significantly higher American College of Rheumatology-20 (ACR20) response rate compared to the placebo group (RR 1.760, 95% CI 1.568–1.977, <i>P</i> < 0.001). Additionally, the risankizumab group showed a significantly higher Minimal Disease Activity (MDA) response rate compared to the placebo group (RR 1.827, 95% CI 1.048–3.184, <i>P</i> < 0.05). The risankizumab group also exhibited improvement in Short Form 36 Questionnaire (SF-36) score (SMD 0.51, 95% CI 0.33–0.69, <i>P</i> < 0.001), with significantly lower Health Assessment Questionnaire Disability Index (HAQ-DI) score (SMD − 0.27, 95% CI − 0.37 to − 0.17, <i>P</i> < 0.001) and higher Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) score (SMD 0.27, 95% CI 0.20–0.35, <i>P</i> < 0.001) compared to the placebo group. Moreover, the risankizumab group had a significantly lower Psoriasis Area and Severity Index (PASI) score (SMD − 6.12, 95% CI − 10.02 to 2.23, <i>P</i> < 0.001). A study by Mease et al. indicated that patients receiving risankizumab generally demonstrated numerical improvements in the Leeds Enthesitis Index (LEI), although the small sample size limits the evidence. Further research is necessary to provide evidence-based guidelines. There were no significant differences in the incidence of serious adverse events (SAE) and serious treatment-emergent adverse events (STEAE) between the risankizumab and placebo groups (RR 0.76, 95% CI 0.45–1.28, <i>P</i> = 0.31; RR 0.99, 95% CI 0.49–1.99, <i>P</i> = 0.97, respectively), and the overall incidence of adverse events (AE) was not comparable (RR 1.10, 95% CI 0.63–1.94, <i>P</i> = 0.73).</p><h3 data-test=\\\"abstract-sub-heading\\\">Conclusion</h3><p>Risankizumab showed superior efficacy across multiple outcome measures compared to placebo, with no significant increase in adverse events. Our findings endorse risankizumab as an excellent treatment option for PsA, offering valuable insights for clinicians and patients when choosing appropriate therapeutic interventions.</p><h3 data-test=\\\"abstract-sub-heading\\\">Trial Registration</h3><p>Retrospectively registered (CRD42023451894, 16 August 2023).</p>\",\"PeriodicalId\":21267,\"journal\":{\"name\":\"Rheumatology and Therapy\",\"volume\":\"46 1\",\"pages\":\"\"},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2024-02-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Rheumatology and Therapy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s40744-024-00638-5\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"RHEUMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Rheumatology and Therapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40744-024-00638-5","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
导言目前,银屑病关节炎(PsA)的病因不明,现有药物治疗的效果也不尽如人意。2019年3月,美国食品和药物管理局(FDA)批准了针对白细胞介素(IL)-23的p19亚基的人源化免疫球蛋白G1(IgG1)单克隆抗体利桑珠单抗用于治疗成人PsA。本研究旨在对双盲、随机、安慰剂对照试验进行荟萃分析,以评估利桑珠单抗在中重度PsA中的有效性和安全性。方法我们对相关数据库进行了全面检索,检索时间为数据库建立至2023年10月1日。我们使用Stata 12.0进行了荟萃分析,并使用I2和Egger检验来评估研究之间的异质性和发表偏倚。偏倚评估使用 Revman5.4 软件生成的偏倚风险图和偏倚风险汇总图进行。综述方案已在PROSPERO(CRD42023451894)上注册,并遵守了系统评价首选报告项目(PRISMA)指南。结果分析纳入了6项随机对照试验(RCT),涉及5038名接受利桑单抗或安慰剂治疗的PsA患者。在24周时,利桑单抗组的美国风湿病学会-20(ACR20)反应率明显高于安慰剂组(RR 1.760,95% CI 1.568-1.977,P <0.001)。此外,与安慰剂组相比,利桑珠单抗组的最小疾病活动度(MDA)反应率明显更高(RR 1.827,95% CI 1.048-3.184,P <0.05)。利桑单抗组的简表 36 问卷(SF-36)得分也有所改善(SMD 0.51,95% CI 0.33-0.69,P <0.001),健康评估问卷残疾指数(HAQ-DI)得分显著降低(SMD - 0.27,95% CI - 0.37 to - 0.17,P <0.001),与安慰剂组相比,慢性疾病治疗功能评估-疲劳(FACIT-F)评分更高(SMD 0.27,95% CI 0.20-0.35,P <0.001)。此外,利桑单抗组的银屑病面积和严重程度指数(PASI)评分也明显降低(SMD - 6.12,95% CI - 10.02 - 2.23,P <0.001)。Mease等人的一项研究表明,接受利桑单抗治疗的患者的利兹腱鞘炎指数(Leeds Enthesitis Index,LEI)普遍有数值上的改善,但由于样本量较小,证据有限。有必要开展进一步研究,以提供循证指南。利桑单抗组和安慰剂组的严重不良事件(SAE)和严重治疗突发不良事件(STEAE)发生率无明显差异(RR 0.76,95% CI 0.45-1.28,P = 0.31;RR 0.99,95% CI 0.49-1.99,P = 0.结论与安慰剂相比,利抗珠单抗在多个结局指标上显示出更优越的疗效,且不良事件无显著增加。我们的研究结果认可利桑单抗是治疗PsA的最佳选择,为临床医生和患者选择适当的治疗干预措施提供了宝贵的见解。试验注册回顾性注册(CRD42023451894,2023年8月16日)。
Efficacy and Safety of Risankizumab in Patients with Psoriatic Arthritis: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Introduction
Currently, the cause of psoriatic arthritis (PsA) is unknown, and the effectiveness of current drug treatments is unsatisfactory. In March 2019, the US Food and Drug Administration (FDA) approved risankizumab, a humanized immunoglobulin G1 (IgG1) monoclonal antibody targeting the p19 subunit of interleukin (IL)-23, for the treatment of PsA in adults. This study aimed to conduct a meta-analysis of double-blind, randomized, placebo-controlled trials to evaluate the effectiveness and safety of risankizumab in moderate-to-severe PsA.
Methods
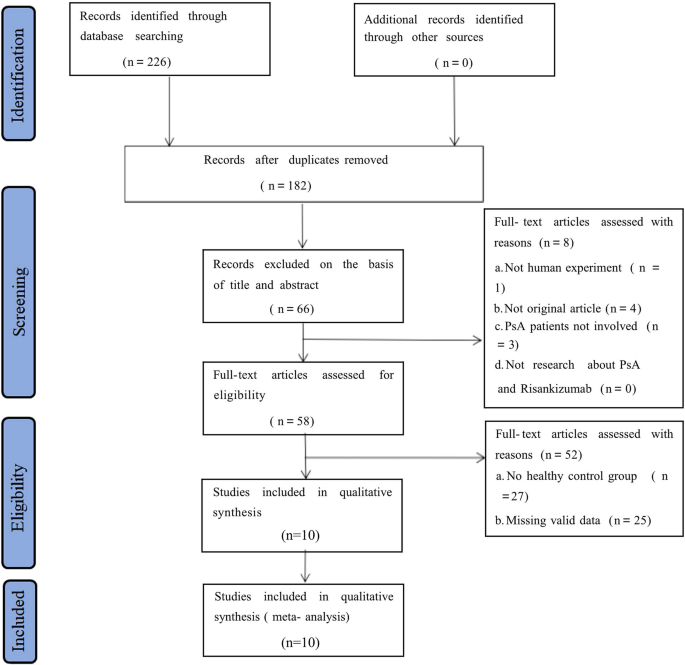
We conducted a thorough search of relevant databases from the establishment of the databases to October 1, 2023. We conducted a meta-analysis using Stata 12.0 and utilized I2 and Egger tests to assess heterogeneity and publication bias among the studies. Bias assessment was performed using the risk bias map and bias risk summary diagram generated by Revman5.4 software. The review protocols were registered on PROSPERO (CRD42023451894) and adhered to the preferred reporting item of system evaluation (PRISMA) guideline.
Results
Six randomized controlled trials (RCTs) involving 5038 patients with PsA treated with either risankizumab or placebo were included in the analysis. At 24 weeks, the risankizumab group demonstrated a significantly higher American College of Rheumatology-20 (ACR20) response rate compared to the placebo group (RR 1.760, 95% CI 1.568–1.977, P < 0.001). Additionally, the risankizumab group showed a significantly higher Minimal Disease Activity (MDA) response rate compared to the placebo group (RR 1.827, 95% CI 1.048–3.184, P < 0.05). The risankizumab group also exhibited improvement in Short Form 36 Questionnaire (SF-36) score (SMD 0.51, 95% CI 0.33–0.69, P < 0.001), with significantly lower Health Assessment Questionnaire Disability Index (HAQ-DI) score (SMD − 0.27, 95% CI − 0.37 to − 0.17, P < 0.001) and higher Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) score (SMD 0.27, 95% CI 0.20–0.35, P < 0.001) compared to the placebo group. Moreover, the risankizumab group had a significantly lower Psoriasis Area and Severity Index (PASI) score (SMD − 6.12, 95% CI − 10.02 to 2.23, P < 0.001). A study by Mease et al. indicated that patients receiving risankizumab generally demonstrated numerical improvements in the Leeds Enthesitis Index (LEI), although the small sample size limits the evidence. Further research is necessary to provide evidence-based guidelines. There were no significant differences in the incidence of serious adverse events (SAE) and serious treatment-emergent adverse events (STEAE) between the risankizumab and placebo groups (RR 0.76, 95% CI 0.45–1.28, P = 0.31; RR 0.99, 95% CI 0.49–1.99, P = 0.97, respectively), and the overall incidence of adverse events (AE) was not comparable (RR 1.10, 95% CI 0.63–1.94, P = 0.73).
Conclusion
Risankizumab showed superior efficacy across multiple outcome measures compared to placebo, with no significant increase in adverse events. Our findings endorse risankizumab as an excellent treatment option for PsA, offering valuable insights for clinicians and patients when choosing appropriate therapeutic interventions.
Trial Registration
Retrospectively registered (CRD42023451894, 16 August 2023).
期刊介绍:
Aims and Scope
Rheumatology and Therapy is an international, open access, peer reviewed, rapid publication journal dedicated to the publication of high-quality clinical (all phases), observational, real-world and health outcomes research around the discovery, development, and use of rheumatologic therapies. Studies relating to diagnosis, pharmacoeconomics, public health, quality of life, and patient care, management, and education are also welcomed.
Areas of focus include, but are not limited to, rheumatoid arthritis, gout, gouty arthritis, psoriatic arthritis, osteoarthritis, juvenile idiopathic/rheumatoid arthritis, systemic lupus erythematosus, axial spondyloarthritis, Pompe’s disease, inflammatory joint conditions, musculoskeletal conditions, systemic sclerosis, and fibromyalgia.
The journal is of interest to a broad audience of healthcare professionals and publishes original research, reviews, case reports, trial protocols, communications and letters. The journal is read by a global audience and receives submissions from all over the world. Rheumatology and Therapy will consider all scientifically sound research be it positive, confirmatory or negative data. Submissions are welcomed whether they relate to an international and/or a country-specific audience, something that is crucially important when researchers are trying to target more specific patient populations. This inclusive approach allows the journal to assist in the dissemination of all scientifically and ethically sound research.
Ethics and Disclosures
The journal is a member of the Committee on Publication Ethics (COPE) and subscribes to its principles on how to deal with acts of misconduct thereby committing to investigate allegations of misconduct in order to ensure the integrity of research. Content in this journal is peer-reviewed (Single-blind). For more information on our publishing ethics policies, please see here: https://www.springer.com/gp/editorial-policies
Rapid Publication
The journal’s rapid publication timelines aim for a peer review decision within 2 weeks of submission. If an article is accepted it will be published online 3-4 weeks from acceptance. These rapid timelines are achieved through the combination of a dedicated in-house editorial team, who closely manage article workflow, and an extensive Editorial and Advisory Board who assist with rapid peer review. This allows the journal to support the rapid dissemination of research, whilst still providing robust peer review. Combined with the journal’s open access model this allows for the rapid and efficient communication of the latest research and reviews, allowing the advancement of rheumatologic therapies.
Personal Service
The journal’s dedicated in-house editorial team offer a personal “concierge service” meaning that authors will always have a personal point of contact able to update them on the status of their manuscript. The editorial team check all manuscripts to ensure that articles conform to the most recent COPE, GPP and ICMJE publishing guidelines. This supports the publication of ethically sound and transparent research. We also encourage pre-submission enquiries and are always happy to provide a confidential assessment of manuscripts.
Digital Features
Rheumatology and Therapy offers a range of additional features designed to increase the visibility, readership and educational value of the journal’s content. Each article is accompanied by key summary points, giving a time-efficient overview of the content to a wide readership. Articles may be accompanied by plain language summaries to assist readers who have some knowledge of, but not in-depth expertise in, the area to understand the scientific content and overall implications of the article. The journal also provides the option to include various types of digital features including animated abstracts, video abstracts, slide decks, audio slides, instructional videos, infographics, podcasts and animations. All additional features are peer reviewed to the same high standard as the article itself. If you consider that your paper would benefit from the inclusion of a digital feature, please let us know. Our editorial team are able to create high-quality slide decks and infographics in-house, and video abstracts through our partner Research Square, and would be happy to assist in any way we can. For further information about digital features, please contact the journal editor (see ‘Contact the Journal’ for email address), and see the ‘Guidelines for digital features and plain language summaries’ document under ‘Submission guidelines’.
For examples of digital features please visit:
https://springerhealthcare.com/expertise/publishing-digital-features/
Preprints
We encourage posting of preprints of primary research manuscripts on preprint servers, authors'' or institutional websites, and open communications between researchers whether on community preprint servers or preprint commenting platforms. Posting of preprints is not considered prior publication and will not jeopardize consideration in our journals. Authors should disclose details of preprint posting during the submission process or at any other point during consideration in the journal. Once the manuscript is published, it is the author''s responsibility to ensure that the preprint record is updated with a publication reference, including the DOI and a URL link to the published version of the article on the journal website.
Please see here for further information on preprint sharing: https://www.springer.com/gp/authors-editors/journal-author/journal-author-helpdesk/submission/1302#c16721550
Peer Review Process
Upon submission, manuscripts are assessed by the editorial team to ensure they fit within the aims and scope of the journal and are also checked for plagiarism. All suitable submissions are then subject to a comprehensive single-blind peer review. Reviewers are selected based on their relevant expertise and publication history in the subject area. The journal has an extensive pool of editorial and advisory board members who have been selected to assist with peer review based on the afore-mentioned criteria.
At least two extensive reviews are required to make the editorial decision. Where reviewer recommendations are conflicted, the editorial board will be contacted for further advice and a presiding decision. Manuscripts are then either accepted, rejected or authors are required to make major or minor revisions (both reviewer comments and editorial comments may need to be addressed). Once a revised manuscript is re-submitted, it is assessed along with the responses to reviewer comments and if it has been adequately revised it will be accepted for publication. Accepted manuscripts are then copyedited and typeset by the production team before online publication. Appeals against decisions following peer review are considered on a case-by-case basis and should be sent to the journal editor, and authors are welcome to make rebuttals against individual reviewer comments if appropriate.
Considering the time and effort required for a detailed peer review we reward our regular reviewers with the opportunity to publish without publication fees (pending peer review) for every three reviews completed per calendar year.
Copyright
Rheumatology and Therapy is published under the Creative Commons Attribution-Noncommercial License, which allows users to read, copy, distribute, and make derivative works for non-commercial purposes from the material, as long as the author of the original work is cited. The author assigns the exclusive right to any commercial use of the article to Springer. For more information about the Creative Commons Attribution-Noncommercial License, click here: http://creativecommons.org/licenses/by-nc/4.0.
Publication Fees
Upon acceptance of an article, authors will be required to pay the mandatory Rapid Service Fee of €5,250/$6,000/£4,300. The journal will consider fee discounts and waivers for developing countries and this is decided on a case-by-case basis.
Open Access
All articles published by Rheumatology and Therapy are published open access.
Contact
For more information about the journal, including pre-submission enquiries, please contact charlotte.maddocks@springernature.com.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


