Iris E Cuperus, Irene M J Mathijssen, Marie-Lise C van Veelen, Anouar Bouzariouh, Ingrid Stubelius, Lars Kölby, Christopher Lundborg, Sumit Das, David Johnson, Steven A Wall, Dawid F Larysz, Krzysztof Dowgierd, Małgorzata Koszowska, Matthias Schulz, Alexander Gratopp, Ulrich-Wilhelm Thomale, Víctor Zafra Vallejo, Marta Redondo Alamillos, Rubén Ferreras Vega, Michela Apolito, Estelle Vergnaud, Giovanna Paternoster, Roman H Khonsari
{"title":"欧洲多中心结果研究:综合颅畸形中面手术后不同围手术期气道管理政策:标准操作程序建议。","authors":"Iris E Cuperus, Irene M J Mathijssen, Marie-Lise C van Veelen, Anouar Bouzariouh, Ingrid Stubelius, Lars Kölby, Christopher Lundborg, Sumit Das, David Johnson, Steven A Wall, Dawid F Larysz, Krzysztof Dowgierd, Małgorzata Koszowska, Matthias Schulz, Alexander Gratopp, Ulrich-Wilhelm Thomale, Víctor Zafra Vallejo, Marta Redondo Alamillos, Rubén Ferreras Vega, Michela Apolito, Estelle Vergnaud, Giovanna Paternoster, Roman H Khonsari","doi":"10.1097/PRS.0000000000011317","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Perioperative airway management following midface advancements in children with Apert and Crouzon-Pfeiffer syndromes can be challenging, and protocols often differ. This study examined airway management following midface advancements and postoperative respiratory complications.</p><p><strong>Methods: </strong>A multicenter, retrospective cohort study was performed to obtain information about the timing of extubation, perioperative airway management, and respiratory complications after monobloc or Le Fort III procedures.</p><p><strong>Results: </strong>A total of 275 patients (monobloc surgery, n = 129; Le Fort III surgery, n = 146) were included. Sixty-two patients received immediate extubation and 162 received delayed extubation; 42 had long-term tracheostomies, and 9 had perioperative short-term tracheostomies. In most centers, short-term tracheostomies were reserved for selected cases. Patients with delayed extubation remained intubated for 3 days (interquartile range, 2 to 5 days). The rate of no or only oxygen support after extubation was comparable between immediate and delayed extubation groups (58 of 62 patients [94%] and 137 of 162 patients [85%], respectively). However, the immediate extubation group developed fewer cases of postoperative pneumonia than did the delayed group (0 of 62 [0%] versus 24 of 161 [15%]; P = 0.001). Immediate extubation also appeared safe in moderate to severe obstructive sleep apnea, as 19 of 20 patients (95%) required either no or only oxygen support after extubation. The odds of developing intubation-related complications increased by 21% with every extra day of intubation.</p><p><strong>Conclusions: </strong>Immediate extubation following midface advancements was found to be a safe option, as it was not associated with respiratory insufficiency but did lead to fewer complications. Immediate extubation should be considered routine management in patients with no or mild obstructive sleep apnea, and should be the aim in moderate to severe obstructive sleep apnea cases after careful assessment.</p><p><strong>Clinical question/level of evidence: </strong>Therapeutic, III.</p>","PeriodicalId":20128,"journal":{"name":"Plastic and reconstructive surgery","volume":" ","pages":"1281-1292"},"PeriodicalIF":3.4000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11584185/pdf/","citationCount":"0","resultStr":"{\"title\":\"A European Multicenter Outcome Study of Perioperative Airway Management Policies following Midface Surgery in Syndromic Craniosynostosis.\",\"authors\":\"Iris E Cuperus, Irene M J Mathijssen, Marie-Lise C van Veelen, Anouar Bouzariouh, Ingrid Stubelius, Lars Kölby, Christopher Lundborg, Sumit Das, David Johnson, Steven A Wall, Dawid F Larysz, Krzysztof Dowgierd, Małgorzata Koszowska, Matthias Schulz, Alexander Gratopp, Ulrich-Wilhelm Thomale, Víctor Zafra Vallejo, Marta Redondo Alamillos, Rubén Ferreras Vega, Michela Apolito, Estelle Vergnaud, Giovanna Paternoster, Roman H Khonsari\",\"doi\":\"10.1097/PRS.0000000000011317\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Perioperative airway management following midface advancements in children with Apert and Crouzon-Pfeiffer syndromes can be challenging, and protocols often differ. This study examined airway management following midface advancements and postoperative respiratory complications.</p><p><strong>Methods: </strong>A multicenter, retrospective cohort study was performed to obtain information about the timing of extubation, perioperative airway management, and respiratory complications after monobloc or Le Fort III procedures.</p><p><strong>Results: </strong>A total of 275 patients (monobloc surgery, n = 129; Le Fort III surgery, n = 146) were included. Sixty-two patients received immediate extubation and 162 received delayed extubation; 42 had long-term tracheostomies, and 9 had perioperative short-term tracheostomies. In most centers, short-term tracheostomies were reserved for selected cases. Patients with delayed extubation remained intubated for 3 days (interquartile range, 2 to 5 days). The rate of no or only oxygen support after extubation was comparable between immediate and delayed extubation groups (58 of 62 patients [94%] and 137 of 162 patients [85%], respectively). However, the immediate extubation group developed fewer cases of postoperative pneumonia than did the delayed group (0 of 62 [0%] versus 24 of 161 [15%]; P = 0.001). Immediate extubation also appeared safe in moderate to severe obstructive sleep apnea, as 19 of 20 patients (95%) required either no or only oxygen support after extubation. The odds of developing intubation-related complications increased by 21% with every extra day of intubation.</p><p><strong>Conclusions: </strong>Immediate extubation following midface advancements was found to be a safe option, as it was not associated with respiratory insufficiency but did lead to fewer complications. Immediate extubation should be considered routine management in patients with no or mild obstructive sleep apnea, and should be the aim in moderate to severe obstructive sleep apnea cases after careful assessment.</p><p><strong>Clinical question/level of evidence: </strong>Therapeutic, III.</p>\",\"PeriodicalId\":20128,\"journal\":{\"name\":\"Plastic and reconstructive surgery\",\"volume\":\" \",\"pages\":\"1281-1292\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2024-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11584185/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Plastic and reconstructive surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1097/PRS.0000000000011317\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Plastic and reconstructive surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1097/PRS.0000000000011317","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/30 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
摘要
背景:阿博特综合征和克鲁宗/菲佛综合征患儿在面中部前移术后的围手术期气道管理可能具有挑战性,而且方案往往各不相同。本研究探讨了面中部前移术后气道管理及术后呼吸系统并发症:方法:进行了一项多中心、回顾性队列研究,以了解单颌/le Fort III 手术后的拔管时机、围术期气道管理和呼吸道并发症:最终纳入了 275 名患者(129 名单体患者和 146 名 Le Fort III 患者);62 名患者接受了立即拔管,162 名患者接受了延迟拔管;42 名患者接受了长期气管造口术,9 名患者在围手术期接受了短期气管造口术。在大多数中心,短期气管造口术只用于特定病例。延迟拔管患者的插管时间为三天(IQR 2 - 5)。立即拔管和延迟拔管患者拔管后无需或仅需氧气支持的比例相当,分别为 58/62 (94%) 和 137/162 (85%)。不过,立即拔管的患者术后肺炎发病率低于延迟拔管的患者,分别为 0/62(0%)对 24/161(15%)(P = 0.001)。对于中度/重度 OSA 患者,立即拔管也显得安全,因为有 19/20 例(95%)患者在拔管后不需要或只需要氧气支持。每多插管一天,发生插管相关并发症的几率就增加21%:结论:研究发现,面中部推进后立即拔管是一种安全的选择,因为它与呼吸功能不全无关,但会导致更少的并发症。对于无/轻度 OSA 患者,应将立即拔管作为常规治疗方法,而对于中度/重度 OSA 患者,则应在仔细评估后将立即拔管作为目标。
A European Multicenter Outcome Study of Perioperative Airway Management Policies following Midface Surgery in Syndromic Craniosynostosis.
Background: Perioperative airway management following midface advancements in children with Apert and Crouzon-Pfeiffer syndromes can be challenging, and protocols often differ. This study examined airway management following midface advancements and postoperative respiratory complications.
Methods: A multicenter, retrospective cohort study was performed to obtain information about the timing of extubation, perioperative airway management, and respiratory complications after monobloc or Le Fort III procedures.
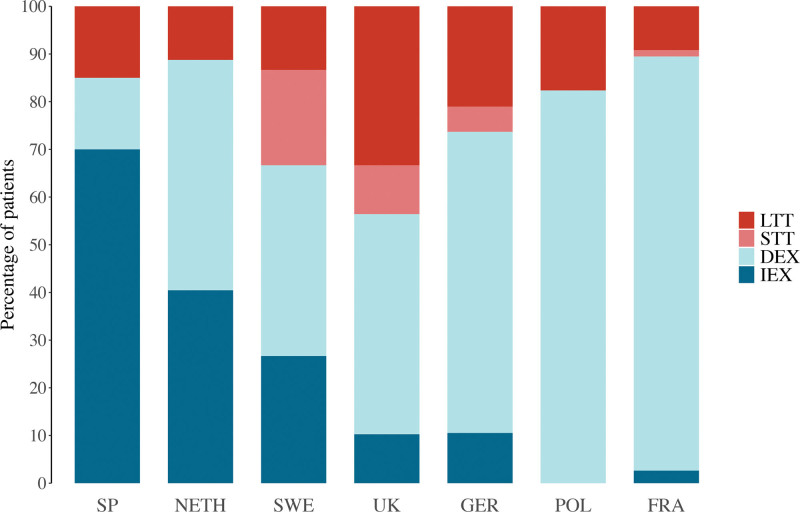
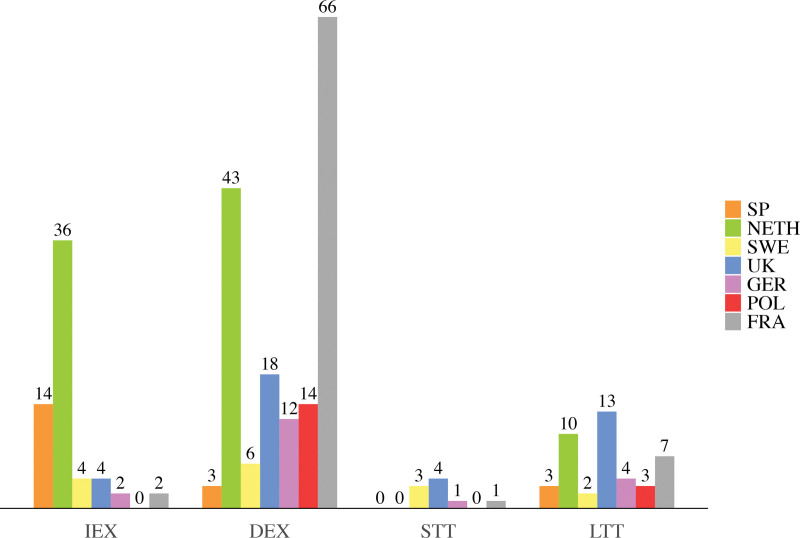
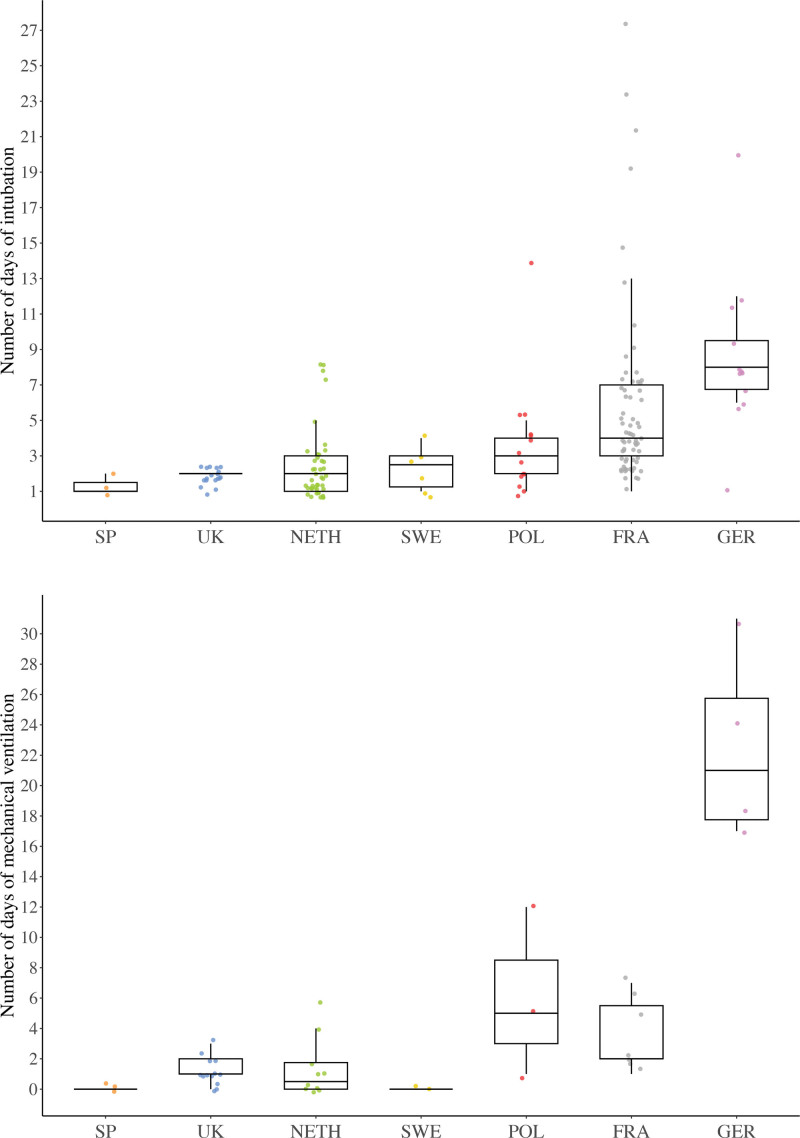
Results: A total of 275 patients (monobloc surgery, n = 129; Le Fort III surgery, n = 146) were included. Sixty-two patients received immediate extubation and 162 received delayed extubation; 42 had long-term tracheostomies, and 9 had perioperative short-term tracheostomies. In most centers, short-term tracheostomies were reserved for selected cases. Patients with delayed extubation remained intubated for 3 days (interquartile range, 2 to 5 days). The rate of no or only oxygen support after extubation was comparable between immediate and delayed extubation groups (58 of 62 patients [94%] and 137 of 162 patients [85%], respectively). However, the immediate extubation group developed fewer cases of postoperative pneumonia than did the delayed group (0 of 62 [0%] versus 24 of 161 [15%]; P = 0.001). Immediate extubation also appeared safe in moderate to severe obstructive sleep apnea, as 19 of 20 patients (95%) required either no or only oxygen support after extubation. The odds of developing intubation-related complications increased by 21% with every extra day of intubation.
Conclusions: Immediate extubation following midface advancements was found to be a safe option, as it was not associated with respiratory insufficiency but did lead to fewer complications. Immediate extubation should be considered routine management in patients with no or mild obstructive sleep apnea, and should be the aim in moderate to severe obstructive sleep apnea cases after careful assessment.
Clinical question/level of evidence: Therapeutic, III.
期刊介绍:
For more than 70 years Plastic and Reconstructive Surgery® has been the one consistently excellent reference for every specialist who uses plastic surgery techniques or works in conjunction with a plastic surgeon. Plastic and Reconstructive Surgery® , the official journal of the American Society of Plastic Surgeons, is a benefit of Society membership, and is also available on a subscription basis.
Plastic and Reconstructive Surgery® brings subscribers up-to-the-minute reports on the latest techniques and follow-up for all areas of plastic and reconstructive surgery, including breast reconstruction, experimental studies, maxillofacial reconstruction, hand and microsurgery, burn repair, cosmetic surgery, as well as news on medicolegal issues. The cosmetic section provides expanded coverage on new procedures and techniques and offers more cosmetic-specific content than any other journal. All subscribers enjoy full access to the Journal''s website, which features broadcast quality videos of reconstructive and cosmetic procedures, podcasts, comprehensive article archives dating to 1946, and additional benefits offered by the newly-redesigned website.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


