Penelope Trimpou, Ioannis Bounias, Olof Ehn, Ola Hammarsten, Oskar Ragnarsson
{"title":"临床实践中 copeptin 的诊断性能:前瞻性研究。","authors":"Penelope Trimpou, Ioannis Bounias, Olof Ehn, Ola Hammarsten, Oskar Ragnarsson","doi":"10.1111/cen.15018","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Objective</h3>\n \n <p>Plasma copeptin is a relatively new biomarker for evaluation of arginine vasopressin (AVP) secretion. The aim of this study was to test the diagnostic performance of copeptin in patients with polyuria-polydipsia syndrome.</p>\n </section>\n \n <section>\n \n <h3> Design, Patients and Measurements</h3>\n \n <p>This was a prospective study where 88 patients with polyuria-polydipsia syndrome were evaluated with a water deprivation test (WDT). Weight, urine osmolality, urine specific gravity, and plasma copeptin were collected at baseline, after 8 h, and at termination of the WDT when one of the following had been reached: (i) >3% weight reduction, (ii) urine specific gravity >1.017 or urine osmolality >600 mOsm/kg, or (iii) intolerable adverse symptoms.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Of 88 patients (57 women), 21 (24%) were diagnosed with central diabetes insipidus (cDI), 5 (6%) with nephrogenic DI (nDI), and 62 (71%) with primary polydipsia (PP). Median (interquartile range) copeptin at baseline was 1.7 (1.4–2.5) pmol/L in cDI, 22 (18–65) pmol/L in nDI, and 2.7 (2–4) pmol/L in PP. After 8 h of WDT, the highest copeptin in patients with cDI was 4.0 pmol/L. In patients with PP: (i) 41 had urine osmolality <600 mOsm/kg, 7 (17%) of these had copeptin >4.0 pmol/L, (ii) 21 had urine osmolality ≥600 mOsm/kg, 14 (67%) of these had copeptin >4.0 pmol/L.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Copeptin >4.0 pmol/L after an overnight WDT can be used to rule out cDI and copeptin ≥21 pmol/L at baseline to diagnose nDI. The diagnostic performance of copeptin in the context of the WDT is otherwise limited in the diagnostic work-up of patients with polyuria-polydipsia syndrome.</p>\n </section>\n </div>","PeriodicalId":10346,"journal":{"name":"Clinical Endocrinology","volume":"101 1","pages":"23-31"},"PeriodicalIF":3.0000,"publicationDate":"2024-01-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/cen.15018","citationCount":"0","resultStr":"{\"title\":\"The diagnostic performance of copeptin in clinical practice: A prospective study\",\"authors\":\"Penelope Trimpou, Ioannis Bounias, Olof Ehn, Ola Hammarsten, Oskar Ragnarsson\",\"doi\":\"10.1111/cen.15018\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Objective</h3>\\n \\n <p>Plasma copeptin is a relatively new biomarker for evaluation of arginine vasopressin (AVP) secretion. The aim of this study was to test the diagnostic performance of copeptin in patients with polyuria-polydipsia syndrome.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Design, Patients and Measurements</h3>\\n \\n <p>This was a prospective study where 88 patients with polyuria-polydipsia syndrome were evaluated with a water deprivation test (WDT). Weight, urine osmolality, urine specific gravity, and plasma copeptin were collected at baseline, after 8 h, and at termination of the WDT when one of the following had been reached: (i) >3% weight reduction, (ii) urine specific gravity >1.017 or urine osmolality >600 mOsm/kg, or (iii) intolerable adverse symptoms.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Of 88 patients (57 women), 21 (24%) were diagnosed with central diabetes insipidus (cDI), 5 (6%) with nephrogenic DI (nDI), and 62 (71%) with primary polydipsia (PP). Median (interquartile range) copeptin at baseline was 1.7 (1.4–2.5) pmol/L in cDI, 22 (18–65) pmol/L in nDI, and 2.7 (2–4) pmol/L in PP. After 8 h of WDT, the highest copeptin in patients with cDI was 4.0 pmol/L. In patients with PP: (i) 41 had urine osmolality <600 mOsm/kg, 7 (17%) of these had copeptin >4.0 pmol/L, (ii) 21 had urine osmolality ≥600 mOsm/kg, 14 (67%) of these had copeptin >4.0 pmol/L.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>Copeptin >4.0 pmol/L after an overnight WDT can be used to rule out cDI and copeptin ≥21 pmol/L at baseline to diagnose nDI. The diagnostic performance of copeptin in the context of the WDT is otherwise limited in the diagnostic work-up of patients with polyuria-polydipsia syndrome.</p>\\n </section>\\n </div>\",\"PeriodicalId\":10346,\"journal\":{\"name\":\"Clinical Endocrinology\",\"volume\":\"101 1\",\"pages\":\"23-31\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2024-01-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/cen.15018\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Endocrinology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/cen.15018\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Endocrinology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/cen.15018","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
The diagnostic performance of copeptin in clinical practice: A prospective study
Objective
Plasma copeptin is a relatively new biomarker for evaluation of arginine vasopressin (AVP) secretion. The aim of this study was to test the diagnostic performance of copeptin in patients with polyuria-polydipsia syndrome.
Design, Patients and Measurements
This was a prospective study where 88 patients with polyuria-polydipsia syndrome were evaluated with a water deprivation test (WDT). Weight, urine osmolality, urine specific gravity, and plasma copeptin were collected at baseline, after 8 h, and at termination of the WDT when one of the following had been reached: (i) >3% weight reduction, (ii) urine specific gravity >1.017 or urine osmolality >600 mOsm/kg, or (iii) intolerable adverse symptoms.
Results
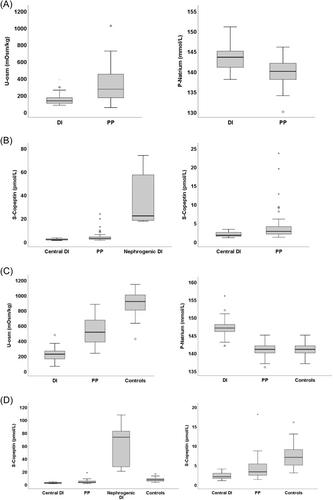
Of 88 patients (57 women), 21 (24%) were diagnosed with central diabetes insipidus (cDI), 5 (6%) with nephrogenic DI (nDI), and 62 (71%) with primary polydipsia (PP). Median (interquartile range) copeptin at baseline was 1.7 (1.4–2.5) pmol/L in cDI, 22 (18–65) pmol/L in nDI, and 2.7 (2–4) pmol/L in PP. After 8 h of WDT, the highest copeptin in patients with cDI was 4.0 pmol/L. In patients with PP: (i) 41 had urine osmolality <600 mOsm/kg, 7 (17%) of these had copeptin >4.0 pmol/L, (ii) 21 had urine osmolality ≥600 mOsm/kg, 14 (67%) of these had copeptin >4.0 pmol/L.
Conclusions
Copeptin >4.0 pmol/L after an overnight WDT can be used to rule out cDI and copeptin ≥21 pmol/L at baseline to diagnose nDI. The diagnostic performance of copeptin in the context of the WDT is otherwise limited in the diagnostic work-up of patients with polyuria-polydipsia syndrome.
期刊介绍:
Clinical Endocrinology publishes papers and reviews which focus on the clinical aspects of endocrinology, including the clinical application of molecular endocrinology. It does not publish papers relating directly to diabetes care and clinical management. It features reviews, original papers, commentaries, correspondence and Clinical Questions. Clinical Endocrinology is essential reading not only for those engaged in endocrinological research but also for those involved primarily in clinical practice.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


