Simroop Ladhar B.Sc, Nathaniel M. Hawkins MBChB, M.D., MPH, Sean A. Virani M.D., M.Sc., MPH, Ricky D. Turgeon Pharm.D.
{"title":"PHARM-HF 是一家由药剂师主导的心力衰竭药物滴定诊所:前后对比研究","authors":"Simroop Ladhar B.Sc, Nathaniel M. Hawkins MBChB, M.D., MPH, Sean A. Virani M.D., M.Sc., MPH, Ricky D. Turgeon Pharm.D.","doi":"10.1002/jac5.1920","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Introduction</h3>\n \n <p>The PHARM-HF clinic is a novel, pharmacist-led medication optimization clinic for patients with heart failure with reduced ejection fraction (HFrEF). PHARM-HF aims to achieve maximum-tolerated HFrEF guideline-directed medical therapy (GDMT) as outlined by the latest Canadian Cardiovascular Society heart failure guidelines.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>This retrospective pre-post study evaluated consecutive patients attending PHARM-HF (January 2021–August 2022). The primary outcome was the modified Optimal Medication Therapy (mOMT) score, an aggregate score of HFrEF quadruple therapy. The mOMT score was categorized as suboptimal (score 0–4), acceptable (score 5–7), or optimal (score 8; all four drugs at maximum tolerated dose). Secondary outcomes included change in left ventricular ejection fraction (LVEF) from baseline to 1 year, and Kansas City Cardiomyopathy Questionnaire-12 (KCCQ; range 0 [worst] to 100 [best]) from baseline to discharge.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Of 81 included patients, median age was 68 years, 21% were female, 61% had New York Heart Association (NYHA) class 2 functional capacity, and median LVEF was 30%. Median mOMT improved from 6 (interquartile range [IQR] 4–7) at baseline to 8 (IQR 7–8) at clinic discharge (<i>p</i> < 0.001; increase from 7% to 73% categorized as optimal). LVEF improved from a median of 30% to 38% at 1 year (<i>p</i> < 0.001). Among 16 patients who completed the KCCQ-12 at both time points, the score was 62 at baseline and 77 at discharge (<i>p</i> = 0.42).</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Uptake of GDMT significantly increased from admission to discharge from the PHARM-HF medication optimization clinic, during which other cardiovascular clinicians did not modify HFrEF medications. Furthermore, there was an improvement in LVEF at 1 year. A pilot randomized controlled trial is currently underway to guide the development of a multicenter trial to provide definitive evidence for the role of pharmacist-led medication optimization in HFrEF.</p>\n </section>\n </div>","PeriodicalId":73966,"journal":{"name":"Journal of the American College of Clinical Pharmacy : JACCP","volume":null,"pages":null},"PeriodicalIF":1.3000,"publicationDate":"2024-01-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jac5.1920","citationCount":"0","resultStr":"{\"title\":\"Evaluation of PHARM-HF, a pharmacist-led heart failure medication titration clinic: A pre-post study\",\"authors\":\"Simroop Ladhar B.Sc, Nathaniel M. Hawkins MBChB, M.D., MPH, Sean A. Virani M.D., M.Sc., MPH, Ricky D. Turgeon Pharm.D.\",\"doi\":\"10.1002/jac5.1920\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Introduction</h3>\\n \\n <p>The PHARM-HF clinic is a novel, pharmacist-led medication optimization clinic for patients with heart failure with reduced ejection fraction (HFrEF). PHARM-HF aims to achieve maximum-tolerated HFrEF guideline-directed medical therapy (GDMT) as outlined by the latest Canadian Cardiovascular Society heart failure guidelines.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>This retrospective pre-post study evaluated consecutive patients attending PHARM-HF (January 2021–August 2022). The primary outcome was the modified Optimal Medication Therapy (mOMT) score, an aggregate score of HFrEF quadruple therapy. The mOMT score was categorized as suboptimal (score 0–4), acceptable (score 5–7), or optimal (score 8; all four drugs at maximum tolerated dose). Secondary outcomes included change in left ventricular ejection fraction (LVEF) from baseline to 1 year, and Kansas City Cardiomyopathy Questionnaire-12 (KCCQ; range 0 [worst] to 100 [best]) from baseline to discharge.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Of 81 included patients, median age was 68 years, 21% were female, 61% had New York Heart Association (NYHA) class 2 functional capacity, and median LVEF was 30%. Median mOMT improved from 6 (interquartile range [IQR] 4–7) at baseline to 8 (IQR 7–8) at clinic discharge (<i>p</i> < 0.001; increase from 7% to 73% categorized as optimal). LVEF improved from a median of 30% to 38% at 1 year (<i>p</i> < 0.001). Among 16 patients who completed the KCCQ-12 at both time points, the score was 62 at baseline and 77 at discharge (<i>p</i> = 0.42).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>Uptake of GDMT significantly increased from admission to discharge from the PHARM-HF medication optimization clinic, during which other cardiovascular clinicians did not modify HFrEF medications. Furthermore, there was an improvement in LVEF at 1 year. A pilot randomized controlled trial is currently underway to guide the development of a multicenter trial to provide definitive evidence for the role of pharmacist-led medication optimization in HFrEF.</p>\\n </section>\\n </div>\",\"PeriodicalId\":73966,\"journal\":{\"name\":\"Journal of the American College of Clinical Pharmacy : JACCP\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2024-01-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jac5.1920\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the American College of Clinical Pharmacy : JACCP\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/jac5.1920\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American College of Clinical Pharmacy : JACCP","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jac5.1920","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
Evaluation of PHARM-HF, a pharmacist-led heart failure medication titration clinic: A pre-post study
Introduction
The PHARM-HF clinic is a novel, pharmacist-led medication optimization clinic for patients with heart failure with reduced ejection fraction (HFrEF). PHARM-HF aims to achieve maximum-tolerated HFrEF guideline-directed medical therapy (GDMT) as outlined by the latest Canadian Cardiovascular Society heart failure guidelines.
Methods
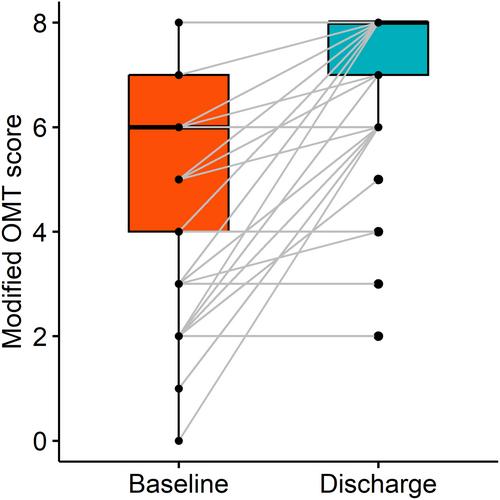
This retrospective pre-post study evaluated consecutive patients attending PHARM-HF (January 2021–August 2022). The primary outcome was the modified Optimal Medication Therapy (mOMT) score, an aggregate score of HFrEF quadruple therapy. The mOMT score was categorized as suboptimal (score 0–4), acceptable (score 5–7), or optimal (score 8; all four drugs at maximum tolerated dose). Secondary outcomes included change in left ventricular ejection fraction (LVEF) from baseline to 1 year, and Kansas City Cardiomyopathy Questionnaire-12 (KCCQ; range 0 [worst] to 100 [best]) from baseline to discharge.
Results
Of 81 included patients, median age was 68 years, 21% were female, 61% had New York Heart Association (NYHA) class 2 functional capacity, and median LVEF was 30%. Median mOMT improved from 6 (interquartile range [IQR] 4–7) at baseline to 8 (IQR 7–8) at clinic discharge (p < 0.001; increase from 7% to 73% categorized as optimal). LVEF improved from a median of 30% to 38% at 1 year (p < 0.001). Among 16 patients who completed the KCCQ-12 at both time points, the score was 62 at baseline and 77 at discharge (p = 0.42).
Conclusions
Uptake of GDMT significantly increased from admission to discharge from the PHARM-HF medication optimization clinic, during which other cardiovascular clinicians did not modify HFrEF medications. Furthermore, there was an improvement in LVEF at 1 year. A pilot randomized controlled trial is currently underway to guide the development of a multicenter trial to provide definitive evidence for the role of pharmacist-led medication optimization in HFrEF.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


