Bruna Barbar, Neomal De Silva, Timothy Cheetham, Claire Wood, Richard Quinton
{"title":"XY 性腺发育不良的性腺肿瘤筛查。","authors":"Bruna Barbar, Neomal De Silva, Timothy Cheetham, Claire Wood, Richard Quinton","doi":"10.1111/cen.15015","DOIUrl":null,"url":null,"abstract":"<p>We read with great interest the recent paper by Hannema et al.<span><sup>1</sup></span> that we found particularly illuminating in respect of our patient with 46XY gonadal dysgenesis, who continues to decline prophylactic gonadectomy.</p><p>Disorders of sex development (DSD) are a group of rare disorders involving abnormalities in karyotype, steroidogenesis, androgen action or gonadal development, resulting in various phenotypic presentations.<span><sup>2</sup></span> Among the genetic determinants of sex development, the <i>SRY</i> (sex-determining region of the Y chromosome) gene initiates development of the male urogenital primordia.<span><sup>2, 3</sup></span> Loss-of-function variants result in congenital abnormalities of male-typical development.</p><p>Swyer syndrome or 46, XY gonadal dysgenesis (46XY GD) presents with female external genitalia and absent puberty due to gonadal insufficiency (hypergonadotrophic hypogonadism). Amidst the potential genetic culprits, variants of the <i>SRY</i> gene account for up to 15% of cases, as specific encoded proteins (i.e.: sex-determining region Y protein HMG-box) bind to regions of deoxyribonucleic acid (DNA) that control male-typical development. Other associated gene loci include <i>MAP3K1, DHH, NR5A1</i> and <i>SOX9</i>.<span><sup>3</sup></span> With no male differentiation stimulus to the urogenital ridge, Sertoli and Leydig cells do not arise within the primitive gonad, resulting in deficiencies of Anti-Müllerian hormone (AMH) and testosterone, respectively. Hence, the development of Mullerian structures and the absence of external male sexual differentiation (Figure 1).</p><p>A 17-year-old female was referred with primary amenorrhoea and absent puberty. Her past medical and family history was insignificant. She had not progressed into puberty (Tanner stage 1) and had normal female external genitalia. Biochemical evaluation revealed hypergonadotrophic hypogonadism (LH—33.7 IU/L, FSH—105.8 IU/L, Oestradiol <60 pmol/L), undetectable Sertoli cell markers and no elevation of tumour markers (AMH < 0.5 pmol/L, Inhibin B < 9.8 ng/L, alpha fetoprotein (AFP) < 1.0 kU/L, carcinoembryonic antigen (CEA) < 1.0 μg/L). Karyotype was 46 XY, indicating gonadal dysgenesis. Magnetic resonance imaging (MRI) scan showed a tiny anteverted uterus (2.9 × 0.6 × 2.0 cm), but no gonads were visualized. The diagnosis had a significant psychological impact on the patient, for which she was signposted to support groups for peer support. She was also referred to clinical psychology through her general practitioner.</p><p>She was then started on transdermal Estradiol at a dose of 6.25 μg twice weekly, gradually up-titrated to achieve normal breast (Tanner 4) and sonographic uterine development, after which she was converted to continuous-combined hormone replacement therapy (currently Estradiol 4 mg plus Norethisterone 1.05 mg daily). Laparoscopic exploration and gonadectomy were also recommended considering the risk of gonadoblastoma, but she firmly declined the procedure and continued to do so over the course of subsequent clinic visits. She remained unconvinced of the need for the procedure as no tumour had yet developed over serial monitoring, despite the increased risk of gonadoblastoma in 46 XY GD having been carefully explained to her.</p><p>Six years after her initial presentation (at 23 years of age), Sertoli cell hormones remained undetectable and a repeat pelvic MRI in 2023 confirmed a mature uterine configuration (62 × 25 × 37 mm), although gonads were again not visualized. The option of exploratory laparoscopy was revisited with input from a gynaecologist, but she remained extremely reluctant to undergo any surgical procedure.</p><p>Phenotypic female patients with DSD have an increased risk of gonadal tumour development in conjunction with the presence of the GBY region of the Y-chromossome.<span><sup>4</sup></span> 46XY pure GD has one of the highest risks of neoplastic transformation in DSD, which is estimated to be around 15<b>%</b>–60<b>%</b>.<span><sup>2</sup></span> Thus, in contrast to other DSDs, having lower neoplasia risk and a chance of undergoing spontaneous puberty, prompt prophylactic gonadectomy is recommended in 46XY GD.</p><p>Although there is a consensus in the literature on the benefits of early bilateral prophylactic gonadectomy, no clear guidance is available regarding the options to pursue when the patient declines this.<span><sup>1, 4, 5</sup></span> Gonadoblastoma is an initially benign tumour that occurs exclusively in dysgenetic gonads, and may then undergo transformation into dysgerminoma, or other malignancy in up to 60% of cases.<span><sup>3</sup></span></p><p>Imaging alone, such as US or MRI, identified 40%–50% of gonads (if present), but failed to identify any of the gonadoblastomas present in 28% of the patients.<span><sup>5</sup></span> Negative imaging was one of the reasons this patient declined the procedure. Clinicians can explain to such patients that imaging has poor sensitivity in identifying gonadoblastomas. Because such methods are not always successful in identifying these tumours, we then explored whether tumour markers and Sertoli cell markers had the potential to identify tumours among those who declined gonadectomy.</p><p>Measurable levels of AMH and inhibin B are correlated with the presence of germ cells, and might therefore indicate a greater potential for tumour development and measurable levels of beta-hCG and AFP might correlate to the presence of some germ cell tumours. Nevertheless, as per the study by Hannema et al.,<span><sup>1</sup></span> the absence of measurable levels of AMH and inhibin B does not exclude the presence of germ cells. They found that 27% of DSD cases with undetectable AMH and/or inhibin B nevertheless had germ cells present in the gonadectomy specimen (all had gonadoblastoma and/or dysgerminoma). Ninety-four percent of patients with detectable inhibin B or AMH presented with germ cells and 35% of them had abnormal germ cells.</p><p>In conclusion, the balance of evidence continues to support prophylactic bilateral gonadectomy in females with 46XY GD, irrespective of Sertoli cell markers. For those women who—despite our best efforts—continue to decline the procedure, the measurement of Sertoli cell markers has poor negative predictive value to reliably exclude the presence of germ cells. Although detectable AMH and inhibin B levels significantly increase the possibility of the presence of germ cells, and hence the risk of gonadoblastoma development, we can counsel patients that their absence by no means precludes the risk. Hopefully this provides an opportunity for these women to re-evaluate their decision. Whereas the majority of affected patients will likely accept medical recommendation to undergo gonadectomy, those who do not should ideally be recruited to the iDSD registry (https://home.i-dsd.org/), so as to gather more data in this area.</p>","PeriodicalId":10346,"journal":{"name":"Clinical Endocrinology","volume":null,"pages":null},"PeriodicalIF":3.0000,"publicationDate":"2024-01-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/cen.15015","citationCount":"0","resultStr":"{\"title\":\"Gonadal tumour screening in XY gonadal dysgenesis\",\"authors\":\"Bruna Barbar, Neomal De Silva, Timothy Cheetham, Claire Wood, Richard Quinton\",\"doi\":\"10.1111/cen.15015\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>We read with great interest the recent paper by Hannema et al.<span><sup>1</sup></span> that we found particularly illuminating in respect of our patient with 46XY gonadal dysgenesis, who continues to decline prophylactic gonadectomy.</p><p>Disorders of sex development (DSD) are a group of rare disorders involving abnormalities in karyotype, steroidogenesis, androgen action or gonadal development, resulting in various phenotypic presentations.<span><sup>2</sup></span> Among the genetic determinants of sex development, the <i>SRY</i> (sex-determining region of the Y chromosome) gene initiates development of the male urogenital primordia.<span><sup>2, 3</sup></span> Loss-of-function variants result in congenital abnormalities of male-typical development.</p><p>Swyer syndrome or 46, XY gonadal dysgenesis (46XY GD) presents with female external genitalia and absent puberty due to gonadal insufficiency (hypergonadotrophic hypogonadism). Amidst the potential genetic culprits, variants of the <i>SRY</i> gene account for up to 15% of cases, as specific encoded proteins (i.e.: sex-determining region Y protein HMG-box) bind to regions of deoxyribonucleic acid (DNA) that control male-typical development. Other associated gene loci include <i>MAP3K1, DHH, NR5A1</i> and <i>SOX9</i>.<span><sup>3</sup></span> With no male differentiation stimulus to the urogenital ridge, Sertoli and Leydig cells do not arise within the primitive gonad, resulting in deficiencies of Anti-Müllerian hormone (AMH) and testosterone, respectively. Hence, the development of Mullerian structures and the absence of external male sexual differentiation (Figure 1).</p><p>A 17-year-old female was referred with primary amenorrhoea and absent puberty. Her past medical and family history was insignificant. She had not progressed into puberty (Tanner stage 1) and had normal female external genitalia. Biochemical evaluation revealed hypergonadotrophic hypogonadism (LH—33.7 IU/L, FSH—105.8 IU/L, Oestradiol <60 pmol/L), undetectable Sertoli cell markers and no elevation of tumour markers (AMH < 0.5 pmol/L, Inhibin B < 9.8 ng/L, alpha fetoprotein (AFP) < 1.0 kU/L, carcinoembryonic antigen (CEA) < 1.0 μg/L). Karyotype was 46 XY, indicating gonadal dysgenesis. Magnetic resonance imaging (MRI) scan showed a tiny anteverted uterus (2.9 × 0.6 × 2.0 cm), but no gonads were visualized. The diagnosis had a significant psychological impact on the patient, for which she was signposted to support groups for peer support. She was also referred to clinical psychology through her general practitioner.</p><p>She was then started on transdermal Estradiol at a dose of 6.25 μg twice weekly, gradually up-titrated to achieve normal breast (Tanner 4) and sonographic uterine development, after which she was converted to continuous-combined hormone replacement therapy (currently Estradiol 4 mg plus Norethisterone 1.05 mg daily). Laparoscopic exploration and gonadectomy were also recommended considering the risk of gonadoblastoma, but she firmly declined the procedure and continued to do so over the course of subsequent clinic visits. She remained unconvinced of the need for the procedure as no tumour had yet developed over serial monitoring, despite the increased risk of gonadoblastoma in 46 XY GD having been carefully explained to her.</p><p>Six years after her initial presentation (at 23 years of age), Sertoli cell hormones remained undetectable and a repeat pelvic MRI in 2023 confirmed a mature uterine configuration (62 × 25 × 37 mm), although gonads were again not visualized. The option of exploratory laparoscopy was revisited with input from a gynaecologist, but she remained extremely reluctant to undergo any surgical procedure.</p><p>Phenotypic female patients with DSD have an increased risk of gonadal tumour development in conjunction with the presence of the GBY region of the Y-chromossome.<span><sup>4</sup></span> 46XY pure GD has one of the highest risks of neoplastic transformation in DSD, which is estimated to be around 15<b>%</b>–60<b>%</b>.<span><sup>2</sup></span> Thus, in contrast to other DSDs, having lower neoplasia risk and a chance of undergoing spontaneous puberty, prompt prophylactic gonadectomy is recommended in 46XY GD.</p><p>Although there is a consensus in the literature on the benefits of early bilateral prophylactic gonadectomy, no clear guidance is available regarding the options to pursue when the patient declines this.<span><sup>1, 4, 5</sup></span> Gonadoblastoma is an initially benign tumour that occurs exclusively in dysgenetic gonads, and may then undergo transformation into dysgerminoma, or other malignancy in up to 60% of cases.<span><sup>3</sup></span></p><p>Imaging alone, such as US or MRI, identified 40%–50% of gonads (if present), but failed to identify any of the gonadoblastomas present in 28% of the patients.<span><sup>5</sup></span> Negative imaging was one of the reasons this patient declined the procedure. Clinicians can explain to such patients that imaging has poor sensitivity in identifying gonadoblastomas. Because such methods are not always successful in identifying these tumours, we then explored whether tumour markers and Sertoli cell markers had the potential to identify tumours among those who declined gonadectomy.</p><p>Measurable levels of AMH and inhibin B are correlated with the presence of germ cells, and might therefore indicate a greater potential for tumour development and measurable levels of beta-hCG and AFP might correlate to the presence of some germ cell tumours. Nevertheless, as per the study by Hannema et al.,<span><sup>1</sup></span> the absence of measurable levels of AMH and inhibin B does not exclude the presence of germ cells. They found that 27% of DSD cases with undetectable AMH and/or inhibin B nevertheless had germ cells present in the gonadectomy specimen (all had gonadoblastoma and/or dysgerminoma). Ninety-four percent of patients with detectable inhibin B or AMH presented with germ cells and 35% of them had abnormal germ cells.</p><p>In conclusion, the balance of evidence continues to support prophylactic bilateral gonadectomy in females with 46XY GD, irrespective of Sertoli cell markers. For those women who—despite our best efforts—continue to decline the procedure, the measurement of Sertoli cell markers has poor negative predictive value to reliably exclude the presence of germ cells. Although detectable AMH and inhibin B levels significantly increase the possibility of the presence of germ cells, and hence the risk of gonadoblastoma development, we can counsel patients that their absence by no means precludes the risk. Hopefully this provides an opportunity for these women to re-evaluate their decision. Whereas the majority of affected patients will likely accept medical recommendation to undergo gonadectomy, those who do not should ideally be recruited to the iDSD registry (https://home.i-dsd.org/), so as to gather more data in this area.</p>\",\"PeriodicalId\":10346,\"journal\":{\"name\":\"Clinical Endocrinology\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2024-01-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/cen.15015\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Endocrinology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/cen.15015\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Endocrinology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/cen.15015","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
摘要
可测量的 AMH 和抑制素 B 水平与生殖细胞的存在相关,因此可能预示着更大的肿瘤发展潜力,而可测量的 β-hCG 和 AFP 水平可能与某些生殖细胞肿瘤的存在相关。然而,根据 Hannema 等人的研究1 ,AMH 和抑制素 B 水平不可测并不排除生殖细胞的存在。他们发现,在检测不到 AMH 和/或抑制素 B 的 DSD 病例中,有 27% 的生殖细胞存在于性腺切除标本中(所有病例都患有性腺母细胞瘤和/或发育不良性生殖细胞瘤)。总之,无论Sertoli细胞标志物如何,平衡证据仍然支持对46XY GD女性进行预防性双侧性腺切除术。尽管我们尽了最大努力,但对于那些继续拒绝接受手术的女性来说,Sertoli细胞标记物的测量结果在可靠排除生殖细胞存在方面的阴性预测价值很低。虽然可检测到的 AMH 和抑制素 B 水平会显著增加生殖细胞存在的可能性,从而增加性腺母细胞瘤发生的风险,但我们可以告知患者,不检测到这两种标志物并不能排除风险。希望这能为这些妇女提供一个重新评估其决定的机会。虽然大多数受影响的患者可能会接受医生的建议,接受性腺切除术,但那些没有接受切除术的患者最好能被招募到 iDSD 登记处 (https://home.i-dsd.org/),以便收集更多这方面的数据。
We read with great interest the recent paper by Hannema et al.1 that we found particularly illuminating in respect of our patient with 46XY gonadal dysgenesis, who continues to decline prophylactic gonadectomy.
Disorders of sex development (DSD) are a group of rare disorders involving abnormalities in karyotype, steroidogenesis, androgen action or gonadal development, resulting in various phenotypic presentations.2 Among the genetic determinants of sex development, the SRY (sex-determining region of the Y chromosome) gene initiates development of the male urogenital primordia.2, 3 Loss-of-function variants result in congenital abnormalities of male-typical development.
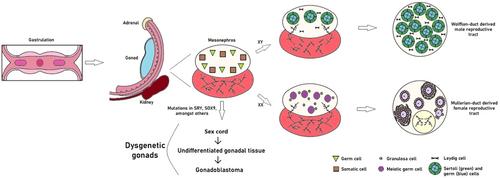
Swyer syndrome or 46, XY gonadal dysgenesis (46XY GD) presents with female external genitalia and absent puberty due to gonadal insufficiency (hypergonadotrophic hypogonadism). Amidst the potential genetic culprits, variants of the SRY gene account for up to 15% of cases, as specific encoded proteins (i.e.: sex-determining region Y protein HMG-box) bind to regions of deoxyribonucleic acid (DNA) that control male-typical development. Other associated gene loci include MAP3K1, DHH, NR5A1 and SOX9.3 With no male differentiation stimulus to the urogenital ridge, Sertoli and Leydig cells do not arise within the primitive gonad, resulting in deficiencies of Anti-Müllerian hormone (AMH) and testosterone, respectively. Hence, the development of Mullerian structures and the absence of external male sexual differentiation (Figure 1).
A 17-year-old female was referred with primary amenorrhoea and absent puberty. Her past medical and family history was insignificant. She had not progressed into puberty (Tanner stage 1) and had normal female external genitalia. Biochemical evaluation revealed hypergonadotrophic hypogonadism (LH—33.7 IU/L, FSH—105.8 IU/L, Oestradiol <60 pmol/L), undetectable Sertoli cell markers and no elevation of tumour markers (AMH < 0.5 pmol/L, Inhibin B < 9.8 ng/L, alpha fetoprotein (AFP) < 1.0 kU/L, carcinoembryonic antigen (CEA) < 1.0 μg/L). Karyotype was 46 XY, indicating gonadal dysgenesis. Magnetic resonance imaging (MRI) scan showed a tiny anteverted uterus (2.9 × 0.6 × 2.0 cm), but no gonads were visualized. The diagnosis had a significant psychological impact on the patient, for which she was signposted to support groups for peer support. She was also referred to clinical psychology through her general practitioner.
She was then started on transdermal Estradiol at a dose of 6.25 μg twice weekly, gradually up-titrated to achieve normal breast (Tanner 4) and sonographic uterine development, after which she was converted to continuous-combined hormone replacement therapy (currently Estradiol 4 mg plus Norethisterone 1.05 mg daily). Laparoscopic exploration and gonadectomy were also recommended considering the risk of gonadoblastoma, but she firmly declined the procedure and continued to do so over the course of subsequent clinic visits. She remained unconvinced of the need for the procedure as no tumour had yet developed over serial monitoring, despite the increased risk of gonadoblastoma in 46 XY GD having been carefully explained to her.
Six years after her initial presentation (at 23 years of age), Sertoli cell hormones remained undetectable and a repeat pelvic MRI in 2023 confirmed a mature uterine configuration (62 × 25 × 37 mm), although gonads were again not visualized. The option of exploratory laparoscopy was revisited with input from a gynaecologist, but she remained extremely reluctant to undergo any surgical procedure.
Phenotypic female patients with DSD have an increased risk of gonadal tumour development in conjunction with the presence of the GBY region of the Y-chromossome.4 46XY pure GD has one of the highest risks of neoplastic transformation in DSD, which is estimated to be around 15%–60%.2 Thus, in contrast to other DSDs, having lower neoplasia risk and a chance of undergoing spontaneous puberty, prompt prophylactic gonadectomy is recommended in 46XY GD.
Although there is a consensus in the literature on the benefits of early bilateral prophylactic gonadectomy, no clear guidance is available regarding the options to pursue when the patient declines this.1, 4, 5 Gonadoblastoma is an initially benign tumour that occurs exclusively in dysgenetic gonads, and may then undergo transformation into dysgerminoma, or other malignancy in up to 60% of cases.3
Imaging alone, such as US or MRI, identified 40%–50% of gonads (if present), but failed to identify any of the gonadoblastomas present in 28% of the patients.5 Negative imaging was one of the reasons this patient declined the procedure. Clinicians can explain to such patients that imaging has poor sensitivity in identifying gonadoblastomas. Because such methods are not always successful in identifying these tumours, we then explored whether tumour markers and Sertoli cell markers had the potential to identify tumours among those who declined gonadectomy.
Measurable levels of AMH and inhibin B are correlated with the presence of germ cells, and might therefore indicate a greater potential for tumour development and measurable levels of beta-hCG and AFP might correlate to the presence of some germ cell tumours. Nevertheless, as per the study by Hannema et al.,1 the absence of measurable levels of AMH and inhibin B does not exclude the presence of germ cells. They found that 27% of DSD cases with undetectable AMH and/or inhibin B nevertheless had germ cells present in the gonadectomy specimen (all had gonadoblastoma and/or dysgerminoma). Ninety-four percent of patients with detectable inhibin B or AMH presented with germ cells and 35% of them had abnormal germ cells.
In conclusion, the balance of evidence continues to support prophylactic bilateral gonadectomy in females with 46XY GD, irrespective of Sertoli cell markers. For those women who—despite our best efforts—continue to decline the procedure, the measurement of Sertoli cell markers has poor negative predictive value to reliably exclude the presence of germ cells. Although detectable AMH and inhibin B levels significantly increase the possibility of the presence of germ cells, and hence the risk of gonadoblastoma development, we can counsel patients that their absence by no means precludes the risk. Hopefully this provides an opportunity for these women to re-evaluate their decision. Whereas the majority of affected patients will likely accept medical recommendation to undergo gonadectomy, those who do not should ideally be recruited to the iDSD registry (https://home.i-dsd.org/), so as to gather more data in this area.
期刊介绍:
Clinical Endocrinology publishes papers and reviews which focus on the clinical aspects of endocrinology, including the clinical application of molecular endocrinology. It does not publish papers relating directly to diabetes care and clinical management. It features reviews, original papers, commentaries, correspondence and Clinical Questions. Clinical Endocrinology is essential reading not only for those engaged in endocrinological research but also for those involved primarily in clinical practice.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


