Areej Salim, Sajid Ali, Muhammad Ali Sheikh, Tariq Latif, Islah Ud Din
{"title":"紧急血管栓塞术治疗威尔姆斯肿瘤危及生命的出血。","authors":"Areej Salim, Sajid Ali, Muhammad Ali Sheikh, Tariq Latif, Islah Ud Din","doi":"10.37029/jcas.v10i1.603","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Renal artery embolization has been used in a palliative fashion for symptomatic relief of hematuria or flank pain in unresectable renal cell carcinoma in adults. There is limited data on the use of embolization for actively bleeding and unresectable tumors in the oncological pediatric population.</p><p><strong>Case description: </strong>A previously healthy 5-year-old boy with no significant past medical or surgical history presented to the clinic with gradually worsening abdominal distension associated with occasional abdominal pain, gross hematuria, and lethargy for four months. Diagnostic investigations showed an 18-cm left-sided metastatic (pulmonary) renal tumor (Wilms), which was deemed unresectable on imaging. Treatment was planned according to the SIOP-RTSG protocol. However, he became hemodynamically and vitally unstable with acute, sudden distension of the abdomen on the left side after the first cycle of chemotherapy. Imaging showed active bleeding from an inferior branch of the left renal artery. Selective angioembolization was done, and chemotherapy was reinitiated with a patent left main renal artery. Following the fourth cycle of chemotherapy, he developed hemodynamic instability and abdominal pain; imaging revealed the resolution of pulmonary nodules and bleeding from the left renal artery (main); this was again embolized, and the patient was stabilized. The patient was operated on after optimization, and a complete resection of the mass was done with negative margins. On six months follow-up, he is well.</p><p><strong>Practical implications: </strong>To the best of our knowledge, this is the first case where angioembolization has been done in conjunction with neoadjuvant chemotherapy to downsize a Wilms tumor to achieve favorable outcomes. Continued research efforts are necessary to optimize strategies and improve the prognosis for pediatric patients, and this case is one of the prime examples.</p>","PeriodicalId":73631,"journal":{"name":"Journal of cancer & allied specialties","volume":"10 1","pages":"603"},"PeriodicalIF":0.0000,"publicationDate":"2024-01-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10793714/pdf/","citationCount":"0","resultStr":"{\"title\":\"Emergency Angioembolization for Life-Threatening Hemorrhage in Wilms Tumor.\",\"authors\":\"Areej Salim, Sajid Ali, Muhammad Ali Sheikh, Tariq Latif, Islah Ud Din\",\"doi\":\"10.37029/jcas.v10i1.603\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Renal artery embolization has been used in a palliative fashion for symptomatic relief of hematuria or flank pain in unresectable renal cell carcinoma in adults. There is limited data on the use of embolization for actively bleeding and unresectable tumors in the oncological pediatric population.</p><p><strong>Case description: </strong>A previously healthy 5-year-old boy with no significant past medical or surgical history presented to the clinic with gradually worsening abdominal distension associated with occasional abdominal pain, gross hematuria, and lethargy for four months. Diagnostic investigations showed an 18-cm left-sided metastatic (pulmonary) renal tumor (Wilms), which was deemed unresectable on imaging. Treatment was planned according to the SIOP-RTSG protocol. However, he became hemodynamically and vitally unstable with acute, sudden distension of the abdomen on the left side after the first cycle of chemotherapy. Imaging showed active bleeding from an inferior branch of the left renal artery. Selective angioembolization was done, and chemotherapy was reinitiated with a patent left main renal artery. Following the fourth cycle of chemotherapy, he developed hemodynamic instability and abdominal pain; imaging revealed the resolution of pulmonary nodules and bleeding from the left renal artery (main); this was again embolized, and the patient was stabilized. The patient was operated on after optimization, and a complete resection of the mass was done with negative margins. On six months follow-up, he is well.</p><p><strong>Practical implications: </strong>To the best of our knowledge, this is the first case where angioembolization has been done in conjunction with neoadjuvant chemotherapy to downsize a Wilms tumor to achieve favorable outcomes. Continued research efforts are necessary to optimize strategies and improve the prognosis for pediatric patients, and this case is one of the prime examples.</p>\",\"PeriodicalId\":73631,\"journal\":{\"name\":\"Journal of cancer & allied specialties\",\"volume\":\"10 1\",\"pages\":\"603\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-01-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10793714/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of cancer & allied specialties\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.37029/jcas.v10i1.603\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of cancer & allied specialties","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.37029/jcas.v10i1.603","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Emergency Angioembolization for Life-Threatening Hemorrhage in Wilms Tumor.
Introduction: Renal artery embolization has been used in a palliative fashion for symptomatic relief of hematuria or flank pain in unresectable renal cell carcinoma in adults. There is limited data on the use of embolization for actively bleeding and unresectable tumors in the oncological pediatric population.
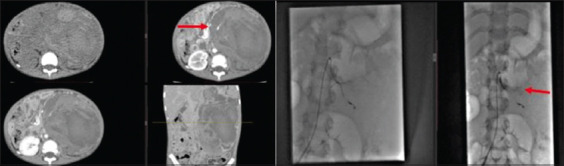
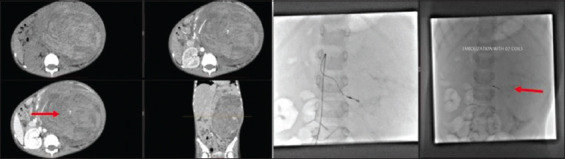
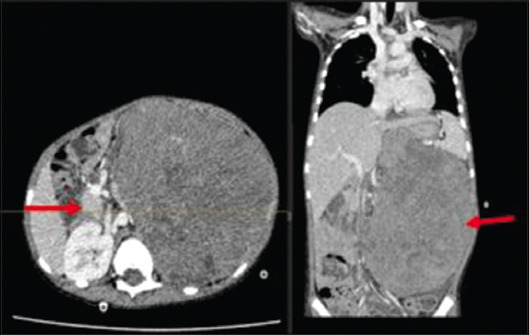
Case description: A previously healthy 5-year-old boy with no significant past medical or surgical history presented to the clinic with gradually worsening abdominal distension associated with occasional abdominal pain, gross hematuria, and lethargy for four months. Diagnostic investigations showed an 18-cm left-sided metastatic (pulmonary) renal tumor (Wilms), which was deemed unresectable on imaging. Treatment was planned according to the SIOP-RTSG protocol. However, he became hemodynamically and vitally unstable with acute, sudden distension of the abdomen on the left side after the first cycle of chemotherapy. Imaging showed active bleeding from an inferior branch of the left renal artery. Selective angioembolization was done, and chemotherapy was reinitiated with a patent left main renal artery. Following the fourth cycle of chemotherapy, he developed hemodynamic instability and abdominal pain; imaging revealed the resolution of pulmonary nodules and bleeding from the left renal artery (main); this was again embolized, and the patient was stabilized. The patient was operated on after optimization, and a complete resection of the mass was done with negative margins. On six months follow-up, he is well.
Practical implications: To the best of our knowledge, this is the first case where angioembolization has been done in conjunction with neoadjuvant chemotherapy to downsize a Wilms tumor to achieve favorable outcomes. Continued research efforts are necessary to optimize strategies and improve the prognosis for pediatric patients, and this case is one of the prime examples.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


