{"title":"可预测二尖瓣狭窄患者压力多普勒超声心动图呼吸困难的收缩肺动脉压力阈值","authors":"Saléha Lehachi, Fadila Daimellah, Saida Khelil, Zakia Bennoui, Djohar Hannoun, Youcef Laid, Rachid Mechmeche, Mohand Said Issad","doi":"10.37616/2212-5043.1354","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>On Stress Doppler Echocardiography (SDE) in mitral stenosis, the systolic pulmonary artery pressure (SPAP) threshold at peak exercise recommended by the guidelines as an indication for percutaneous mitral commissurotomy (PMC) used to be 60 mmHg. However, because of the paucity of studies, that threshold has been controversial. The Europeans stopped using the value in 2007, followed by the Americans in 2014.</p><p><strong>Objective: </strong>Determine SPAP thresholds on SDE at peak exercise and post-exercise predictive of dyspnea as an indication for PMC in mitral stenosis.</p><p><strong>Method and results: </strong>Three hundred mitral stenosis patients with a mitral valve area (MVA) ≤ 2 cm<sup>2</sup> and NYHA I-II-III were included. A treadmill stress test (Bruce protocol) was used in all cases to distinguish dyspneic patients (n = 182) from non dyspneic patients (n = 118). SDE was performed on a stress echocardiography bed, starting at 30 W and increasing by 30 W every 3 min. At peak exercise, the best SPAP threshold obtained was 75 mmHg: specificity (Sp) = 0.98 (0.94-1), positive likelihood ratio (LR+) = 47 (41-50), positive predictive value (PPV) = 0.99 (0.95-1), and positive predictive error (PPE) = 0.01 (0.002-0.05). This compared with, respectively, 0.34, 1, 0.69 and 0.31 at 60 mmHg. Post-exercise, the best SPAP threshold found was 60 mmHg: Sp = .94 (0.88-0.97), LR = 9 (4-10), PPV = 0.94 (0.87-0.97), and PPE = 0.06 (0.03-0.13).</p><p><strong>Conclusion: </strong>Regarding the prediction of dyspnea as an indication for PMC, our study shows that a SPAP value at peak exercise of 60 mmHg lacks predictive power (LR+=1). The optimal threshold observed was 75 mmHg at peak exercise (LR+ = 47 [41-50]) and 60 mmHg post-exercise (LR+ = 9 [4-10]).</p>","PeriodicalId":17319,"journal":{"name":"Journal of the Saudi Heart Association","volume":"35 4","pages":"354-362"},"PeriodicalIF":1.3000,"publicationDate":"2024-01-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10803005/pdf/","citationCount":"0","resultStr":"{\"title\":\"Systolic Pulmonary Artery Pressure Thresholds Predictive of Dyspnea on Stress Doppler Echocardiography in Mitral Stenosis.\",\"authors\":\"Saléha Lehachi, Fadila Daimellah, Saida Khelil, Zakia Bennoui, Djohar Hannoun, Youcef Laid, Rachid Mechmeche, Mohand Said Issad\",\"doi\":\"10.37616/2212-5043.1354\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>On Stress Doppler Echocardiography (SDE) in mitral stenosis, the systolic pulmonary artery pressure (SPAP) threshold at peak exercise recommended by the guidelines as an indication for percutaneous mitral commissurotomy (PMC) used to be 60 mmHg. However, because of the paucity of studies, that threshold has been controversial. The Europeans stopped using the value in 2007, followed by the Americans in 2014.</p><p><strong>Objective: </strong>Determine SPAP thresholds on SDE at peak exercise and post-exercise predictive of dyspnea as an indication for PMC in mitral stenosis.</p><p><strong>Method and results: </strong>Three hundred mitral stenosis patients with a mitral valve area (MVA) ≤ 2 cm<sup>2</sup> and NYHA I-II-III were included. A treadmill stress test (Bruce protocol) was used in all cases to distinguish dyspneic patients (n = 182) from non dyspneic patients (n = 118). SDE was performed on a stress echocardiography bed, starting at 30 W and increasing by 30 W every 3 min. At peak exercise, the best SPAP threshold obtained was 75 mmHg: specificity (Sp) = 0.98 (0.94-1), positive likelihood ratio (LR+) = 47 (41-50), positive predictive value (PPV) = 0.99 (0.95-1), and positive predictive error (PPE) = 0.01 (0.002-0.05). This compared with, respectively, 0.34, 1, 0.69 and 0.31 at 60 mmHg. Post-exercise, the best SPAP threshold found was 60 mmHg: Sp = .94 (0.88-0.97), LR = 9 (4-10), PPV = 0.94 (0.87-0.97), and PPE = 0.06 (0.03-0.13).</p><p><strong>Conclusion: </strong>Regarding the prediction of dyspnea as an indication for PMC, our study shows that a SPAP value at peak exercise of 60 mmHg lacks predictive power (LR+=1). The optimal threshold observed was 75 mmHg at peak exercise (LR+ = 47 [41-50]) and 60 mmHg post-exercise (LR+ = 9 [4-10]).</p>\",\"PeriodicalId\":17319,\"journal\":{\"name\":\"Journal of the Saudi Heart Association\",\"volume\":\"35 4\",\"pages\":\"354-362\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2024-01-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10803005/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the Saudi Heart Association\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.37616/2212-5043.1354\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Saudi Heart Association","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.37616/2212-5043.1354","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Systolic Pulmonary Artery Pressure Thresholds Predictive of Dyspnea on Stress Doppler Echocardiography in Mitral Stenosis.
Background: On Stress Doppler Echocardiography (SDE) in mitral stenosis, the systolic pulmonary artery pressure (SPAP) threshold at peak exercise recommended by the guidelines as an indication for percutaneous mitral commissurotomy (PMC) used to be 60 mmHg. However, because of the paucity of studies, that threshold has been controversial. The Europeans stopped using the value in 2007, followed by the Americans in 2014.
Objective: Determine SPAP thresholds on SDE at peak exercise and post-exercise predictive of dyspnea as an indication for PMC in mitral stenosis.
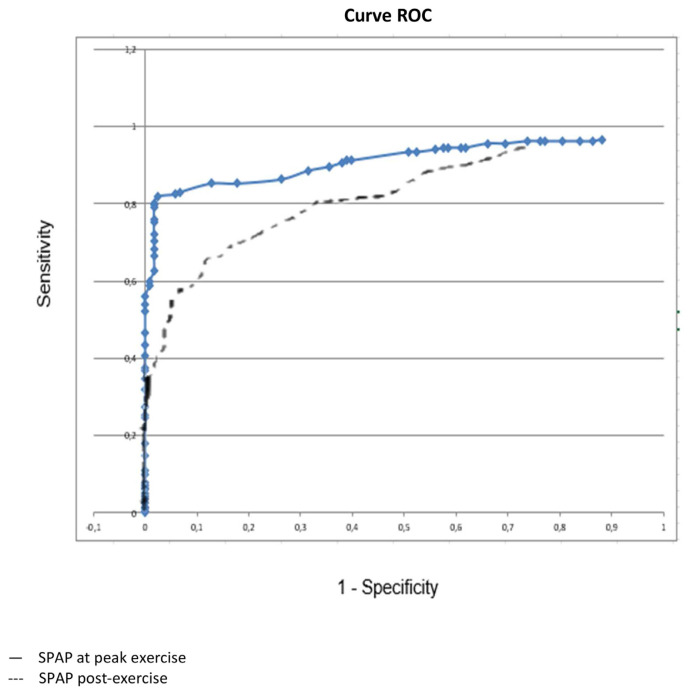
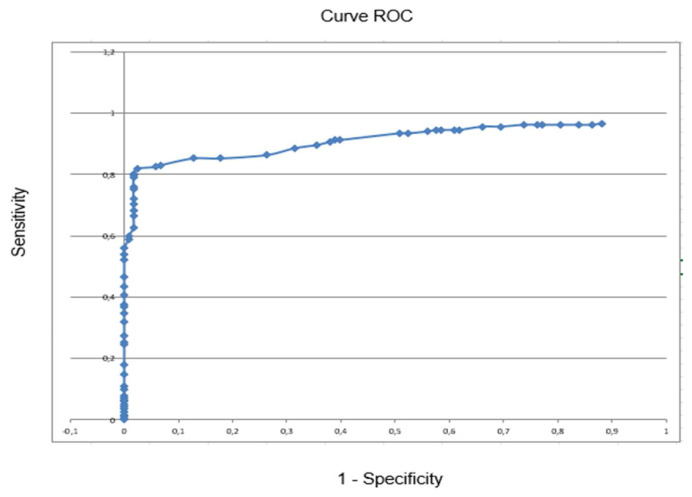
Method and results: Three hundred mitral stenosis patients with a mitral valve area (MVA) ≤ 2 cm2 and NYHA I-II-III were included. A treadmill stress test (Bruce protocol) was used in all cases to distinguish dyspneic patients (n = 182) from non dyspneic patients (n = 118). SDE was performed on a stress echocardiography bed, starting at 30 W and increasing by 30 W every 3 min. At peak exercise, the best SPAP threshold obtained was 75 mmHg: specificity (Sp) = 0.98 (0.94-1), positive likelihood ratio (LR+) = 47 (41-50), positive predictive value (PPV) = 0.99 (0.95-1), and positive predictive error (PPE) = 0.01 (0.002-0.05). This compared with, respectively, 0.34, 1, 0.69 and 0.31 at 60 mmHg. Post-exercise, the best SPAP threshold found was 60 mmHg: Sp = .94 (0.88-0.97), LR = 9 (4-10), PPV = 0.94 (0.87-0.97), and PPE = 0.06 (0.03-0.13).
Conclusion: Regarding the prediction of dyspnea as an indication for PMC, our study shows that a SPAP value at peak exercise of 60 mmHg lacks predictive power (LR+=1). The optimal threshold observed was 75 mmHg at peak exercise (LR+ = 47 [41-50]) and 60 mmHg post-exercise (LR+ = 9 [4-10]).

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


