Edd Maclean, Karishma Mahtani, Shohreh Honarbakhsh, Charles Butcher, Nikhil Ahluwalia, Adam S C Dennis, Antonio Creta, Malcolm Finlay, Mark Elliott, Vishal Mehta, Nadeev Wijesuriya, Omar Shaikh, Yom Zaw, Chizute Ogbedeh, Vasu Gautam, Pier D Lambiase, Richard J Schilling, Mark J Earley, Philip Moore, Amal Muthumala, Simon C E Sporton, Ross J Hunter, Christopher A Rinaldi, Jonathan Behar, Claire Martin, Christopher Monkhouse, Anthony Chow
{"title":"水泡评分:用于预测心脏植入式电子设备感染的新型外部验证工具及其对抗菌包膜使用的成本效益影响。","authors":"Edd Maclean, Karishma Mahtani, Shohreh Honarbakhsh, Charles Butcher, Nikhil Ahluwalia, Adam S C Dennis, Antonio Creta, Malcolm Finlay, Mark Elliott, Vishal Mehta, Nadeev Wijesuriya, Omar Shaikh, Yom Zaw, Chizute Ogbedeh, Vasu Gautam, Pier D Lambiase, Richard J Schilling, Mark J Earley, Philip Moore, Amal Muthumala, Simon C E Sporton, Ross J Hunter, Christopher A Rinaldi, Jonathan Behar, Claire Martin, Christopher Monkhouse, Anthony Chow","doi":"10.1161/CIRCEP.123.012446","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Antimicrobial envelopes reduce the incidence of cardiac implantable electronic device infections, but their cost restricts routine use in the United Kingdom. Risk scoring could help to identify which patients would most benefit from this technology.</p><p><strong>Methods: </strong>A novel risk score (BLISTER [Blood results, Long procedure time, Immunosuppressed, Sixty years old (or younger), Type of procedure, Early re-intervention, Repeat procedure]) was derived from multivariate analysis of factors associated with cardiac implantable electronic device infection. Diagnostic utility was assessed against the existing PADIT score (Prior procedure, Age, Depressed renal function, Immunocompromised, Type of procedure) in both standard and high-risk external validation cohorts, and cost-utility models examined different BLISTER and PADIT score thresholds for TYRX (Medtronic; Minneapolis, MN) antimicrobial envelope allocation.</p><p><strong>Results: </strong>In a derivation cohort (n=7383), cardiac implantable electronic device infection occurred in 59 individuals within 12 months of a procedure (event rate, 0.8%). In addition to the PADIT score constituents, lead extraction (hazard ratio, 3.3 [95% CI, 1.9-6.1]; <i>P</i><0.0001), C-reactive protein >50 mg/L (hazard ratio, 3.0 [95% CI, 1.4-6.4]; <i>P</i>=0.005), reintervention within 2 years (hazard ratio, 10.1 [95% CI, 5.6-17.9]; <i>P</i><0.0001), and top-quartile procedure duration (hazard ratio, 2.6 [95% CI, 1.6-4.1]; <i>P</i>=0.001) were independent predictors of infection. The BLISTER score demonstrated superior discriminative performance versus PADIT in the standard risk (n=2854, event rate: 0.8%, area under the curve, 0.82 versus 0.71; <i>P</i>=0.001) and high-risk validation cohorts (n=1961, event rate: 2.0%, area under the curve, 0.77 versus 0.69; <i>P</i>=0.001), and in all patients (n=12 198, event rate: 1%, area under the curve, 0.8 versus 0.75, <i>P</i>=0.002). In decision-analytic modeling, the optimum scenario assigned antimicrobial envelopes to patients with BLISTER scores ≥6 (10.8%), delivering a significant reduction in infections (relative risk reduction, 30%; <i>P</i>=0.036) within the National Institute for Health and Care Excellence cost-utility thresholds (incremental cost-effectiveness ratio, £18 446).</p><p><strong>Conclusions: </strong>The BLISTER score (https://qxmd.com/calculate/calculator_876/the-blister-score-for-cied-infection) was a valid predictor of cardiac implantable electronic device infection, and could facilitate cost-effective antimicrobial envelope allocation to high-risk patients.</p>","PeriodicalId":10319,"journal":{"name":"Circulation. Arrhythmia and electrophysiology","volume":" ","pages":"e012446"},"PeriodicalIF":9.8000,"publicationDate":"2024-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10949977/pdf/","citationCount":"0","resultStr":"{\"title\":\"The BLISTER Score: A Novel, Externally Validated Tool for Predicting Cardiac Implantable Electronic Device Infections, and Its Cost-Utility Implications for Antimicrobial Envelope Use.\",\"authors\":\"Edd Maclean, Karishma Mahtani, Shohreh Honarbakhsh, Charles Butcher, Nikhil Ahluwalia, Adam S C Dennis, Antonio Creta, Malcolm Finlay, Mark Elliott, Vishal Mehta, Nadeev Wijesuriya, Omar Shaikh, Yom Zaw, Chizute Ogbedeh, Vasu Gautam, Pier D Lambiase, Richard J Schilling, Mark J Earley, Philip Moore, Amal Muthumala, Simon C E Sporton, Ross J Hunter, Christopher A Rinaldi, Jonathan Behar, Claire Martin, Christopher Monkhouse, Anthony Chow\",\"doi\":\"10.1161/CIRCEP.123.012446\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Antimicrobial envelopes reduce the incidence of cardiac implantable electronic device infections, but their cost restricts routine use in the United Kingdom. Risk scoring could help to identify which patients would most benefit from this technology.</p><p><strong>Methods: </strong>A novel risk score (BLISTER [Blood results, Long procedure time, Immunosuppressed, Sixty years old (or younger), Type of procedure, Early re-intervention, Repeat procedure]) was derived from multivariate analysis of factors associated with cardiac implantable electronic device infection. Diagnostic utility was assessed against the existing PADIT score (Prior procedure, Age, Depressed renal function, Immunocompromised, Type of procedure) in both standard and high-risk external validation cohorts, and cost-utility models examined different BLISTER and PADIT score thresholds for TYRX (Medtronic; Minneapolis, MN) antimicrobial envelope allocation.</p><p><strong>Results: </strong>In a derivation cohort (n=7383), cardiac implantable electronic device infection occurred in 59 individuals within 12 months of a procedure (event rate, 0.8%). In addition to the PADIT score constituents, lead extraction (hazard ratio, 3.3 [95% CI, 1.9-6.1]; <i>P</i><0.0001), C-reactive protein >50 mg/L (hazard ratio, 3.0 [95% CI, 1.4-6.4]; <i>P</i>=0.005), reintervention within 2 years (hazard ratio, 10.1 [95% CI, 5.6-17.9]; <i>P</i><0.0001), and top-quartile procedure duration (hazard ratio, 2.6 [95% CI, 1.6-4.1]; <i>P</i>=0.001) were independent predictors of infection. The BLISTER score demonstrated superior discriminative performance versus PADIT in the standard risk (n=2854, event rate: 0.8%, area under the curve, 0.82 versus 0.71; <i>P</i>=0.001) and high-risk validation cohorts (n=1961, event rate: 2.0%, area under the curve, 0.77 versus 0.69; <i>P</i>=0.001), and in all patients (n=12 198, event rate: 1%, area under the curve, 0.8 versus 0.75, <i>P</i>=0.002). In decision-analytic modeling, the optimum scenario assigned antimicrobial envelopes to patients with BLISTER scores ≥6 (10.8%), delivering a significant reduction in infections (relative risk reduction, 30%; <i>P</i>=0.036) within the National Institute for Health and Care Excellence cost-utility thresholds (incremental cost-effectiveness ratio, £18 446).</p><p><strong>Conclusions: </strong>The BLISTER score (https://qxmd.com/calculate/calculator_876/the-blister-score-for-cied-infection) was a valid predictor of cardiac implantable electronic device infection, and could facilitate cost-effective antimicrobial envelope allocation to high-risk patients.</p>\",\"PeriodicalId\":10319,\"journal\":{\"name\":\"Circulation. Arrhythmia and electrophysiology\",\"volume\":\" \",\"pages\":\"e012446\"},\"PeriodicalIF\":9.8000,\"publicationDate\":\"2024-03-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10949977/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Circulation. Arrhythmia and electrophysiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1161/CIRCEP.123.012446\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/22 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Circulation. Arrhythmia and electrophysiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1161/CIRCEP.123.012446","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/22 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
The BLISTER Score: A Novel, Externally Validated Tool for Predicting Cardiac Implantable Electronic Device Infections, and Its Cost-Utility Implications for Antimicrobial Envelope Use.
Background: Antimicrobial envelopes reduce the incidence of cardiac implantable electronic device infections, but their cost restricts routine use in the United Kingdom. Risk scoring could help to identify which patients would most benefit from this technology.
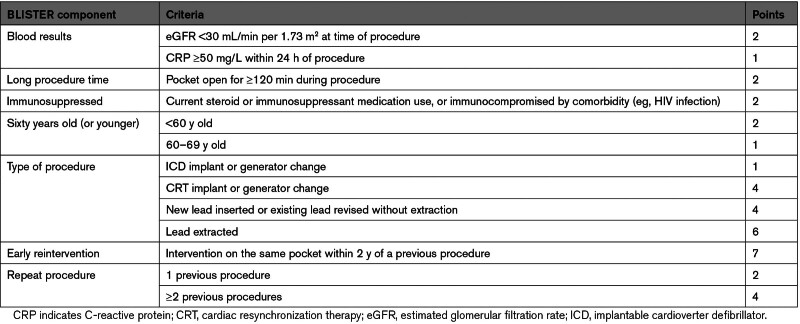
Methods: A novel risk score (BLISTER [Blood results, Long procedure time, Immunosuppressed, Sixty years old (or younger), Type of procedure, Early re-intervention, Repeat procedure]) was derived from multivariate analysis of factors associated with cardiac implantable electronic device infection. Diagnostic utility was assessed against the existing PADIT score (Prior procedure, Age, Depressed renal function, Immunocompromised, Type of procedure) in both standard and high-risk external validation cohorts, and cost-utility models examined different BLISTER and PADIT score thresholds for TYRX (Medtronic; Minneapolis, MN) antimicrobial envelope allocation.
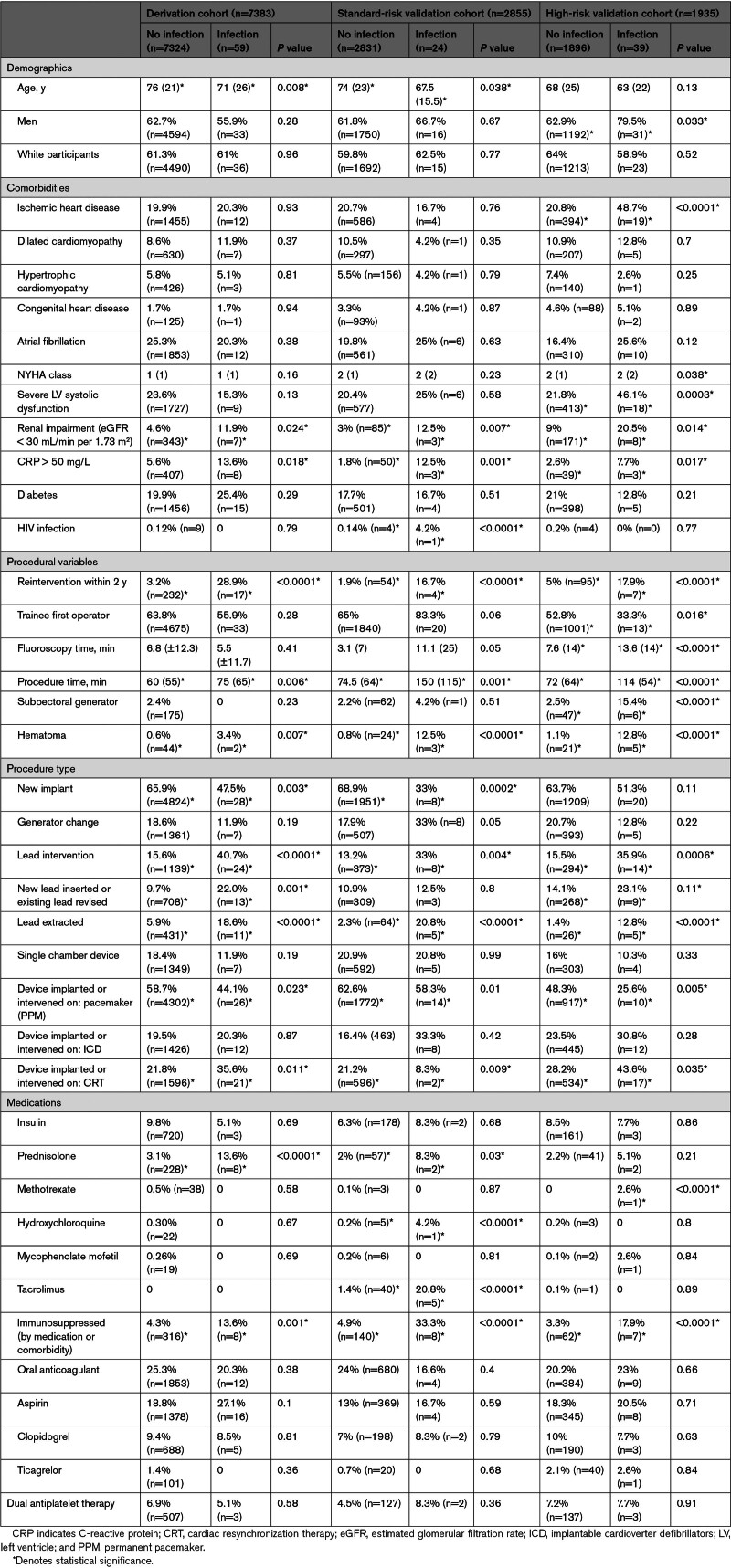
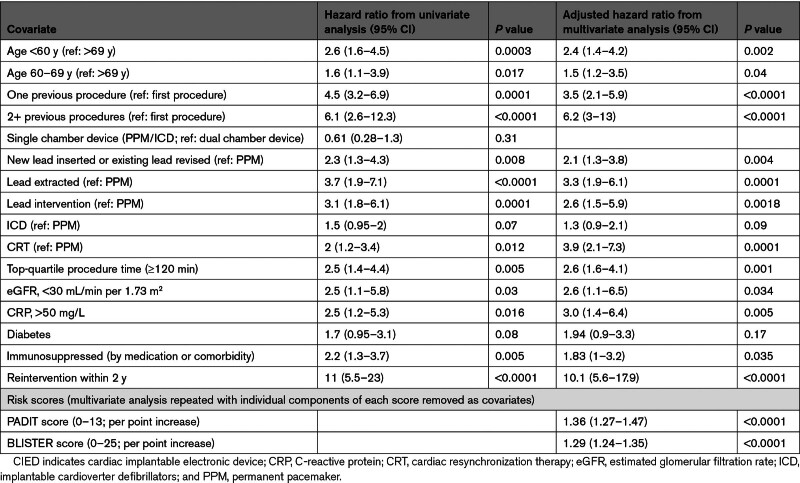
Results: In a derivation cohort (n=7383), cardiac implantable electronic device infection occurred in 59 individuals within 12 months of a procedure (event rate, 0.8%). In addition to the PADIT score constituents, lead extraction (hazard ratio, 3.3 [95% CI, 1.9-6.1]; P<0.0001), C-reactive protein >50 mg/L (hazard ratio, 3.0 [95% CI, 1.4-6.4]; P=0.005), reintervention within 2 years (hazard ratio, 10.1 [95% CI, 5.6-17.9]; P<0.0001), and top-quartile procedure duration (hazard ratio, 2.6 [95% CI, 1.6-4.1]; P=0.001) were independent predictors of infection. The BLISTER score demonstrated superior discriminative performance versus PADIT in the standard risk (n=2854, event rate: 0.8%, area under the curve, 0.82 versus 0.71; P=0.001) and high-risk validation cohorts (n=1961, event rate: 2.0%, area under the curve, 0.77 versus 0.69; P=0.001), and in all patients (n=12 198, event rate: 1%, area under the curve, 0.8 versus 0.75, P=0.002). In decision-analytic modeling, the optimum scenario assigned antimicrobial envelopes to patients with BLISTER scores ≥6 (10.8%), delivering a significant reduction in infections (relative risk reduction, 30%; P=0.036) within the National Institute for Health and Care Excellence cost-utility thresholds (incremental cost-effectiveness ratio, £18 446).
Conclusions: The BLISTER score (https://qxmd.com/calculate/calculator_876/the-blister-score-for-cied-infection) was a valid predictor of cardiac implantable electronic device infection, and could facilitate cost-effective antimicrobial envelope allocation to high-risk patients.
期刊介绍:
Circulation: Arrhythmia and Electrophysiology is a journal dedicated to the study and application of clinical cardiac electrophysiology. It covers a wide range of topics including the diagnosis and treatment of cardiac arrhythmias, as well as research in this field. The journal accepts various types of studies, including observational research, clinical trials, epidemiological studies, and advancements in translational research.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


