{"title":"老年护理中微小结肠炎的诊断和药物治疗。","authors":"Ole Haagen Nielsen, Darrell S Pardi","doi":"10.1007/s40266-023-01094-6","DOIUrl":null,"url":null,"abstract":"<p><p>Microscopic colitis, a diagnosis under the umbrella term of inflammatory bowel disease, is a prevalent cause of watery diarrhea, often with symptoms of urgency and bloating, typically observed in older adults aged ≥ 60 years. Its incidence has been reported to exceed those of ulcerative colitis and Crohn's disease in some geographical areas. Although nonpathognomonic endoscopic abnormalities, including changes of the vascular mucosal pattern; mucosal erythema; edema; nodularity; or mucosal defects, e.g., \"cat scratches\" have been reported, a colonoscopy is typically macroscopically normal. As reliable biomarkers are unavailable, colonoscopy using random biopsies from various parts of the colon is compulsory. Based on the histological examination under a microscope, the disease is divided into collagenous (with a thickened subepithelial collagenous band) and lymphocytic (with intraepithelial lymphocytosis) colitis, although incomplete forms exist. In routine clinical settings, the disease has a high risk of being misdiagnosed as irritable bowel syndrome or even overlooked. Therefore, healthcare providers should be familiar with clinical features and rational management strategies. A 6-8-week oral budesonide treatment course (9 mg/day) is considered the first-line therapy, but patients often experience relapse when discontinued, or might become intolerant, dependent, or even fail to respond. Consequently, other therapeutic options (e.g., bismuth subsalicylate, biologics, loperamide, bile acid sequestrants, and thiopurines) recommended by available guidelines may be prescribed. Herein, clinically meaningful data is provided based on the latest evidence that may aid in reaching a diagnosis and establishing rational therapy in geriatric care to control symptoms and enhance the quality of life for those affected.</p>","PeriodicalId":11489,"journal":{"name":"Drugs & Aging","volume":" ","pages":"113-123"},"PeriodicalIF":3.4000,"publicationDate":"2024-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10869377/pdf/","citationCount":"0","resultStr":"{\"title\":\"Diagnosis and Pharmacological Management of Microscopic Colitis in Geriatric Care.\",\"authors\":\"Ole Haagen Nielsen, Darrell S Pardi\",\"doi\":\"10.1007/s40266-023-01094-6\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Microscopic colitis, a diagnosis under the umbrella term of inflammatory bowel disease, is a prevalent cause of watery diarrhea, often with symptoms of urgency and bloating, typically observed in older adults aged ≥ 60 years. Its incidence has been reported to exceed those of ulcerative colitis and Crohn's disease in some geographical areas. Although nonpathognomonic endoscopic abnormalities, including changes of the vascular mucosal pattern; mucosal erythema; edema; nodularity; or mucosal defects, e.g., \\\"cat scratches\\\" have been reported, a colonoscopy is typically macroscopically normal. As reliable biomarkers are unavailable, colonoscopy using random biopsies from various parts of the colon is compulsory. Based on the histological examination under a microscope, the disease is divided into collagenous (with a thickened subepithelial collagenous band) and lymphocytic (with intraepithelial lymphocytosis) colitis, although incomplete forms exist. In routine clinical settings, the disease has a high risk of being misdiagnosed as irritable bowel syndrome or even overlooked. Therefore, healthcare providers should be familiar with clinical features and rational management strategies. A 6-8-week oral budesonide treatment course (9 mg/day) is considered the first-line therapy, but patients often experience relapse when discontinued, or might become intolerant, dependent, or even fail to respond. Consequently, other therapeutic options (e.g., bismuth subsalicylate, biologics, loperamide, bile acid sequestrants, and thiopurines) recommended by available guidelines may be prescribed. Herein, clinically meaningful data is provided based on the latest evidence that may aid in reaching a diagnosis and establishing rational therapy in geriatric care to control symptoms and enhance the quality of life for those affected.</p>\",\"PeriodicalId\":11489,\"journal\":{\"name\":\"Drugs & Aging\",\"volume\":\" \",\"pages\":\"113-123\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2024-02-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10869377/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Drugs & Aging\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s40266-023-01094-6\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/17 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"GERIATRICS & GERONTOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Drugs & Aging","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40266-023-01094-6","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/17 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
Diagnosis and Pharmacological Management of Microscopic Colitis in Geriatric Care.
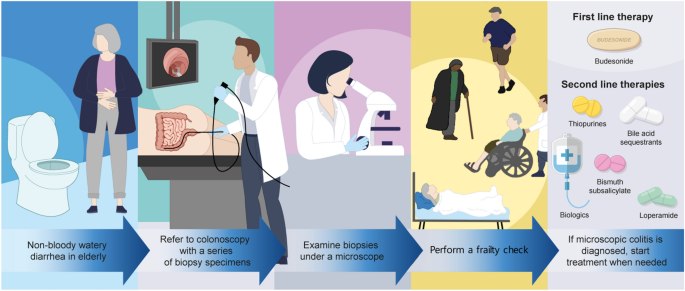
Microscopic colitis, a diagnosis under the umbrella term of inflammatory bowel disease, is a prevalent cause of watery diarrhea, often with symptoms of urgency and bloating, typically observed in older adults aged ≥ 60 years. Its incidence has been reported to exceed those of ulcerative colitis and Crohn's disease in some geographical areas. Although nonpathognomonic endoscopic abnormalities, including changes of the vascular mucosal pattern; mucosal erythema; edema; nodularity; or mucosal defects, e.g., "cat scratches" have been reported, a colonoscopy is typically macroscopically normal. As reliable biomarkers are unavailable, colonoscopy using random biopsies from various parts of the colon is compulsory. Based on the histological examination under a microscope, the disease is divided into collagenous (with a thickened subepithelial collagenous band) and lymphocytic (with intraepithelial lymphocytosis) colitis, although incomplete forms exist. In routine clinical settings, the disease has a high risk of being misdiagnosed as irritable bowel syndrome or even overlooked. Therefore, healthcare providers should be familiar with clinical features and rational management strategies. A 6-8-week oral budesonide treatment course (9 mg/day) is considered the first-line therapy, but patients often experience relapse when discontinued, or might become intolerant, dependent, or even fail to respond. Consequently, other therapeutic options (e.g., bismuth subsalicylate, biologics, loperamide, bile acid sequestrants, and thiopurines) recommended by available guidelines may be prescribed. Herein, clinically meaningful data is provided based on the latest evidence that may aid in reaching a diagnosis and establishing rational therapy in geriatric care to control symptoms and enhance the quality of life for those affected.
期刊介绍:
Drugs & Aging delivers essential information on the most important aspects of drug therapy to professionals involved in the care of the elderly.
The journal addresses in a timely way the major issues relating to drug therapy in older adults including: the management of specific diseases, particularly those associated with aging, age-related physiological changes impacting drug therapy, drug utilization and prescribing in the elderly, polypharmacy and drug interactions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


