Joseph F. Zywiciel BS , Raymond A. Verm MD , Wissam Raad MD , Marshall Baker MD, FACS , Richard Freeman MD, MBA , Zaid M. Abdelsattar MD, MS, FACS
{"title":"涉及胸壁的局部晚期 cT3N2(IIIB 期)肺癌的胸壁内固定切除术:重新审视指南","authors":"Joseph F. Zywiciel BS , Raymond A. Verm MD , Wissam Raad MD , Marshall Baker MD, FACS , Richard Freeman MD, MBA , Zaid M. Abdelsattar MD, MS, FACS","doi":"10.1016/j.xjon.2023.12.007","DOIUrl":null,"url":null,"abstract":"<div><h3>Objectives</h3><p>Current National Comprehensive Cancer Network guidelines recommend definitive chemoradiation rather than surgery for patients with locally advanced clinical stage T3 and N2 (stage IIIB) lung cancer involving the chest wall. The data supporting this recommendation are controversial. We studied whether surgery confers a survival advantage over definitive chemoradiation in the National Cancer Database.</p></div><div><h3>Methods</h3><p>We identified all patients with clinical stage T3 and N2 lung cancer in the National Cancer Database from 2004 to 2017 who underwent a lobectomy with en bloc chest wall resection and compared them with patients with clinical stage T3 and N2 lung cancer who had definitive chemoradiation. We used propensity score matching to minimize confounding by indication while excluding patients with tumors in the upper lobes to exclude Pancoast tumors. We used 1:1 propensity score matching and Kaplan–Meir survival analyses to estimate associations.</p></div><div><h3>Results</h3><p>Of 4467 patients meeting all inclusion/exclusion criteria, 210 (4.49%) had an en bloc chest wall resection. Patients undergoing surgical resection were younger (mean age = 60.3 ± 10.3 years vs 67.5 ± 10.4 years; <em>P</em> < .001) and had more adenocarcinoma (59.0% vs 44.5%; <em>P</em> < .001) but were otherwise similar in terms of sex (37.1% female vs 42.0%; <em>P</em> = .167) and race (Whites 84.3% vs 84.0%; <em>P</em> = .276) compared with the definitive chemoradiation group. After resection, there was an unadjusted 30- and 90-day mortality rate of 3.3% and 9.5%, respectively. A substantial survival benefit with surgical resection persisted after propensity score matching (log-rank <em>P</em> < .001).</p></div><div><h3>Conclusions</h3><p>In this large observational study, we found that in select patients, en bloc chest wall resection for locally advanced clinical stage T3 and N2 lung cancer was associated with improved survival compared with definitive chemoradiation. National Comprehensive Cancer Network guidelines should be revisited.</p></div>","PeriodicalId":74032,"journal":{"name":"JTCVS open","volume":null,"pages":null},"PeriodicalIF":0.0000,"publicationDate":"2024-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S2666273623004242/pdfft?md5=3293b1306bd400e9ba025f2cadfbe7ce&pid=1-s2.0-S2666273623004242-main.pdf","citationCount":"0","resultStr":"{\"title\":\"En bloc chest wall resection in locally advanced cT3N2 (stage IIIB) lung cancer involving the chest wall: Revisiting guidelines\",\"authors\":\"Joseph F. Zywiciel BS , Raymond A. Verm MD , Wissam Raad MD , Marshall Baker MD, FACS , Richard Freeman MD, MBA , Zaid M. Abdelsattar MD, MS, FACS\",\"doi\":\"10.1016/j.xjon.2023.12.007\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Objectives</h3><p>Current National Comprehensive Cancer Network guidelines recommend definitive chemoradiation rather than surgery for patients with locally advanced clinical stage T3 and N2 (stage IIIB) lung cancer involving the chest wall. The data supporting this recommendation are controversial. We studied whether surgery confers a survival advantage over definitive chemoradiation in the National Cancer Database.</p></div><div><h3>Methods</h3><p>We identified all patients with clinical stage T3 and N2 lung cancer in the National Cancer Database from 2004 to 2017 who underwent a lobectomy with en bloc chest wall resection and compared them with patients with clinical stage T3 and N2 lung cancer who had definitive chemoradiation. We used propensity score matching to minimize confounding by indication while excluding patients with tumors in the upper lobes to exclude Pancoast tumors. We used 1:1 propensity score matching and Kaplan–Meir survival analyses to estimate associations.</p></div><div><h3>Results</h3><p>Of 4467 patients meeting all inclusion/exclusion criteria, 210 (4.49%) had an en bloc chest wall resection. Patients undergoing surgical resection were younger (mean age = 60.3 ± 10.3 years vs 67.5 ± 10.4 years; <em>P</em> < .001) and had more adenocarcinoma (59.0% vs 44.5%; <em>P</em> < .001) but were otherwise similar in terms of sex (37.1% female vs 42.0%; <em>P</em> = .167) and race (Whites 84.3% vs 84.0%; <em>P</em> = .276) compared with the definitive chemoradiation group. After resection, there was an unadjusted 30- and 90-day mortality rate of 3.3% and 9.5%, respectively. A substantial survival benefit with surgical resection persisted after propensity score matching (log-rank <em>P</em> < .001).</p></div><div><h3>Conclusions</h3><p>In this large observational study, we found that in select patients, en bloc chest wall resection for locally advanced clinical stage T3 and N2 lung cancer was associated with improved survival compared with definitive chemoradiation. National Comprehensive Cancer Network guidelines should be revisited.</p></div>\",\"PeriodicalId\":74032,\"journal\":{\"name\":\"JTCVS open\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.sciencedirect.com/science/article/pii/S2666273623004242/pdfft?md5=3293b1306bd400e9ba025f2cadfbe7ce&pid=1-s2.0-S2666273623004242-main.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JTCVS open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2666273623004242\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JTCVS open","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2666273623004242","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
目的美国国家综合癌症网络(National Comprehensive Cancer Network)的现行指南建议,对于涉及胸壁的局部晚期临床分期为 T3 和 N2(IIIB 期)的肺癌患者,应进行明确的化疗而非手术治疗。支持这一建议的数据存在争议。我们在全国癌症数据库中研究了手术是否比确定性化疗更具生存优势。方法我们在全国癌症数据库中识别了2004年至2017年所有接受了胸壁全切的肺叶切除术的临床T3期和N2期肺癌患者,并与接受确定性化疗的临床T3期和N2期肺癌患者进行了比较。我们采用倾向得分匹配法来尽量减少适应症的混杂,同时排除上叶肿瘤患者,以排除潘氏肿瘤。我们使用 1:1 倾向性评分匹配和 Kaplan-Meir 生存分析来估计相关性。结果 在 4467 例符合所有纳入/排除标准的患者中,210 例(4.49%)进行了胸壁全切。接受手术切除的患者年龄较小(平均年龄 = 60.3 ± 10.3 岁 vs 67.5 ± 10.4 岁;P < .001),腺癌患者较多(59.0% vs 44.5%;P < .001),但在性别(37.1% 女性 vs 42.0%;P = .167)和种族(白人 84.3% vs 84.0%;P = .276)方面与化疗组相似。切除术后,未经调整的 30 天和 90 天死亡率分别为 3.3% 和 9.5%。结论在这项大型观察性研究中,我们发现与确定性化疗相比,对局部晚期临床分期为 T3 和 N2 的肺癌患者进行胸壁全块切除可提高生存率。应重新审视美国国家综合癌症网络指南。
En bloc chest wall resection in locally advanced cT3N2 (stage IIIB) lung cancer involving the chest wall: Revisiting guidelines
Objectives
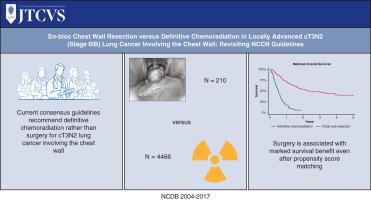
Current National Comprehensive Cancer Network guidelines recommend definitive chemoradiation rather than surgery for patients with locally advanced clinical stage T3 and N2 (stage IIIB) lung cancer involving the chest wall. The data supporting this recommendation are controversial. We studied whether surgery confers a survival advantage over definitive chemoradiation in the National Cancer Database.
Methods
We identified all patients with clinical stage T3 and N2 lung cancer in the National Cancer Database from 2004 to 2017 who underwent a lobectomy with en bloc chest wall resection and compared them with patients with clinical stage T3 and N2 lung cancer who had definitive chemoradiation. We used propensity score matching to minimize confounding by indication while excluding patients with tumors in the upper lobes to exclude Pancoast tumors. We used 1:1 propensity score matching and Kaplan–Meir survival analyses to estimate associations.
Results
Of 4467 patients meeting all inclusion/exclusion criteria, 210 (4.49%) had an en bloc chest wall resection. Patients undergoing surgical resection were younger (mean age = 60.3 ± 10.3 years vs 67.5 ± 10.4 years; P < .001) and had more adenocarcinoma (59.0% vs 44.5%; P < .001) but were otherwise similar in terms of sex (37.1% female vs 42.0%; P = .167) and race (Whites 84.3% vs 84.0%; P = .276) compared with the definitive chemoradiation group. After resection, there was an unadjusted 30- and 90-day mortality rate of 3.3% and 9.5%, respectively. A substantial survival benefit with surgical resection persisted after propensity score matching (log-rank P < .001).
Conclusions
In this large observational study, we found that in select patients, en bloc chest wall resection for locally advanced clinical stage T3 and N2 lung cancer was associated with improved survival compared with definitive chemoradiation. National Comprehensive Cancer Network guidelines should be revisited.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


