{"title":"髓鞘少突胶质细胞糖蛋白抗体相关疾病:概述","authors":"Tatsuro Misu, Yuki Matsumoto, Kimihiko Kaneko, Toshiyuki Takahashi, Yoshiki Takai, Hirohiko Ono, Chihiro Namatame, Shuhei Nishiyama, Juichi Fujimori, Hiroshi Kuroda, Ichiro Nakashima, Kazuo Fujihara, Masashi Aoki","doi":"10.1111/cen3.12771","DOIUrl":null,"url":null,"abstract":"<p>In recent years, there is growing evidence of associations between antibodies against myelin oligodendrocyte glycoprotein (MOG) and several phenotypes of acute inflammatory demyelinating diseases such as acute disseminated encephalomyelitis (ADEM), optic neuritis, brainstem, and cerebral cortical encephalitis, called MOG antibody associated disorders (MOGAD). Monophasic course is known in about half of cases especially in pediatric onset ADEM and optic neuritis, mainly in cases with transient positivity of MOG antibody. Pathological features of MOGAD are considered as acute demyelinating lesions with CD4 dominant cell infiltrations, the deposition of humoral immunity, perivascular inflammation and perivenous demyelination, which is distinct from multiple sclerosis. Now the diagnosis of MOGAD is based on the international panel criteria of MOGAD launched in 2023, which the diagnostic frameworks are three parts, including MOGAD-specific clinical features, MOG antibody positivity, and the exclusion of other diseases. The prognosis of MOGAD patients is considered relatively mild, but the problem is refractory relapsing cases. For its prevention, there are no approved drugs, but oral tapering corticosteroids, immunosuppressants such as azathioprine and mycophenolic mofetil, rituximab, and the maintenance intravenous immunoglobulin are recommended, and now there are a few clinical trials of promising biological drugs already approved in other neurological disorders.</p>","PeriodicalId":10193,"journal":{"name":"Clinical and Experimental Neuroimmunology","volume":"15 1","pages":"6-15"},"PeriodicalIF":0.0000,"publicationDate":"2023-12-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/cen3.12771","citationCount":"0","resultStr":"{\"title\":\"Myelin oligodendrocyte glycoprotein antibody-associated disorders: An overview\",\"authors\":\"Tatsuro Misu, Yuki Matsumoto, Kimihiko Kaneko, Toshiyuki Takahashi, Yoshiki Takai, Hirohiko Ono, Chihiro Namatame, Shuhei Nishiyama, Juichi Fujimori, Hiroshi Kuroda, Ichiro Nakashima, Kazuo Fujihara, Masashi Aoki\",\"doi\":\"10.1111/cen3.12771\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>In recent years, there is growing evidence of associations between antibodies against myelin oligodendrocyte glycoprotein (MOG) and several phenotypes of acute inflammatory demyelinating diseases such as acute disseminated encephalomyelitis (ADEM), optic neuritis, brainstem, and cerebral cortical encephalitis, called MOG antibody associated disorders (MOGAD). Monophasic course is known in about half of cases especially in pediatric onset ADEM and optic neuritis, mainly in cases with transient positivity of MOG antibody. Pathological features of MOGAD are considered as acute demyelinating lesions with CD4 dominant cell infiltrations, the deposition of humoral immunity, perivascular inflammation and perivenous demyelination, which is distinct from multiple sclerosis. Now the diagnosis of MOGAD is based on the international panel criteria of MOGAD launched in 2023, which the diagnostic frameworks are three parts, including MOGAD-specific clinical features, MOG antibody positivity, and the exclusion of other diseases. The prognosis of MOGAD patients is considered relatively mild, but the problem is refractory relapsing cases. For its prevention, there are no approved drugs, but oral tapering corticosteroids, immunosuppressants such as azathioprine and mycophenolic mofetil, rituximab, and the maintenance intravenous immunoglobulin are recommended, and now there are a few clinical trials of promising biological drugs already approved in other neurological disorders.</p>\",\"PeriodicalId\":10193,\"journal\":{\"name\":\"Clinical and Experimental Neuroimmunology\",\"volume\":\"15 1\",\"pages\":\"6-15\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-12-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/cen3.12771\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical and Experimental Neuroimmunology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/cen3.12771\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"Immunology and Microbiology\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Experimental Neuroimmunology","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/cen3.12771","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"Immunology and Microbiology","Score":null,"Total":0}
Myelin oligodendrocyte glycoprotein antibody-associated disorders: An overview
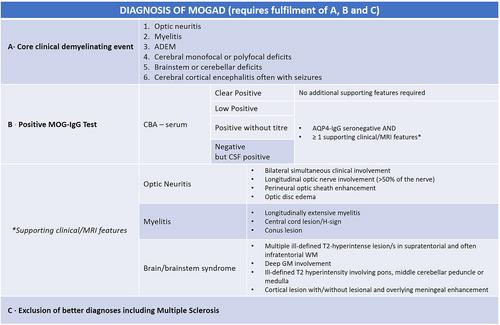
In recent years, there is growing evidence of associations between antibodies against myelin oligodendrocyte glycoprotein (MOG) and several phenotypes of acute inflammatory demyelinating diseases such as acute disseminated encephalomyelitis (ADEM), optic neuritis, brainstem, and cerebral cortical encephalitis, called MOG antibody associated disorders (MOGAD). Monophasic course is known in about half of cases especially in pediatric onset ADEM and optic neuritis, mainly in cases with transient positivity of MOG antibody. Pathological features of MOGAD are considered as acute demyelinating lesions with CD4 dominant cell infiltrations, the deposition of humoral immunity, perivascular inflammation and perivenous demyelination, which is distinct from multiple sclerosis. Now the diagnosis of MOGAD is based on the international panel criteria of MOGAD launched in 2023, which the diagnostic frameworks are three parts, including MOGAD-specific clinical features, MOG antibody positivity, and the exclusion of other diseases. The prognosis of MOGAD patients is considered relatively mild, but the problem is refractory relapsing cases. For its prevention, there are no approved drugs, but oral tapering corticosteroids, immunosuppressants such as azathioprine and mycophenolic mofetil, rituximab, and the maintenance intravenous immunoglobulin are recommended, and now there are a few clinical trials of promising biological drugs already approved in other neurological disorders.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


