Ning Huang, Jihui Zhou, Wan Lu, Laipeng Luo, Huizhen Yuan, Lu Pan, Shujun Ding, Bicheng Yang, Yanqiu Liu
{"title":"X 染色体易位的特征和临床评估。","authors":"Ning Huang, Jihui Zhou, Wan Lu, Laipeng Luo, Huizhen Yuan, Lu Pan, Shujun Ding, Bicheng Yang, Yanqiu Liu","doi":"10.1186/s13039-023-00669-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Individuals with X chromosomal translocations, variable phenotypes, and a high risk of live birth defects are of interest for scientific study. These characteristics are related to differential breakpoints and various types of chromosomal abnormalities. To investigate the effects of X chromosome translocation on clinical phenotype, a retrospective analysis of clinical data for patients with X chromosome translocation was conducted. Karyotype analysis plus endocrine evaluation was utilized for all the patients. Additional semen analysis and Y chromosome microdeletions were assessed in male patients.</p><p><strong>Results: </strong>X chromosome translocations were detected in ten cases, including seven females and three males. Infantile uterus and no ovaries were detected in case 1 (FSH: 114 IU/L, LH: 30.90 mIU/mL, E2: < 5.00 pg/ml), and the karyotype was confirmed as 46,X,t(X;22)(q25;q11.2) in case 1. Infantile uterus and small ovaries were both visible in two cases (FSH: 34.80 IU/L, LH: 17.06 mIU/mL, E2: 15.37 pg/ml in case 2; FISH: 6.60 IU/L, LH: 1.69 mIU/mL, E2: 23.70 pg/ml in case 3). The karyotype was detected as 46,X,t(X;8)(q13;q11.2) in case 2 and 46,X,der(X)t(X;5)(q21;q31) in case 3. Normal reproductive hormone levels and fertility abilities were found for cases 4, 6 and 7. The karyotype were detected as 46,X,t(X;5)(p22.3;q22) in case 4 and 46,X,der(X)t(X;Y)(p22.3;q11.2) in cases 6 and 7. These patients exhibited unremarkable clinical manifestations but experienced a history of abnormal chromosomal pregnancy. Normal phenotype and a complex reciprocal translocation as 46,X,t(X;14;4)(q24;q22;q33) were observed in case 5 with a history of spontaneous abortions. In the three male patients, multiple semen analyses confirmed the absence of sperm. Y chromosome microdeletion and hormonal analyses were normal. The karyotypes were detected as 46,Y,t(X;8)(q26;q22), 46,Y,t(X;1)(q26;q23), 46,Y,t(X;3)(q26;p24), respectively.</p><p><strong>Conclusions: </strong>Our study provides insights into individuals with X chromosome translocations. The clinical phenotypes are variable and unpredictable due to differences in breakpoints and X chromosome inactivation (XCI) patterns. Our results suggest that physicians should focus on the characteristics of the X chromosome translocations and provide personalized clinical evaluations in genetic counselling.</p>","PeriodicalId":19099,"journal":{"name":"Molecular Cytogenetics","volume":"16 1","pages":"36"},"PeriodicalIF":1.4000,"publicationDate":"2023-12-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10740294/pdf/","citationCount":"0","resultStr":"{\"title\":\"Characteristics and clinical evaluation of X chromosome translocations.\",\"authors\":\"Ning Huang, Jihui Zhou, Wan Lu, Laipeng Luo, Huizhen Yuan, Lu Pan, Shujun Ding, Bicheng Yang, Yanqiu Liu\",\"doi\":\"10.1186/s13039-023-00669-7\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Individuals with X chromosomal translocations, variable phenotypes, and a high risk of live birth defects are of interest for scientific study. These characteristics are related to differential breakpoints and various types of chromosomal abnormalities. To investigate the effects of X chromosome translocation on clinical phenotype, a retrospective analysis of clinical data for patients with X chromosome translocation was conducted. Karyotype analysis plus endocrine evaluation was utilized for all the patients. Additional semen analysis and Y chromosome microdeletions were assessed in male patients.</p><p><strong>Results: </strong>X chromosome translocations were detected in ten cases, including seven females and three males. Infantile uterus and no ovaries were detected in case 1 (FSH: 114 IU/L, LH: 30.90 mIU/mL, E2: < 5.00 pg/ml), and the karyotype was confirmed as 46,X,t(X;22)(q25;q11.2) in case 1. Infantile uterus and small ovaries were both visible in two cases (FSH: 34.80 IU/L, LH: 17.06 mIU/mL, E2: 15.37 pg/ml in case 2; FISH: 6.60 IU/L, LH: 1.69 mIU/mL, E2: 23.70 pg/ml in case 3). The karyotype was detected as 46,X,t(X;8)(q13;q11.2) in case 2 and 46,X,der(X)t(X;5)(q21;q31) in case 3. Normal reproductive hormone levels and fertility abilities were found for cases 4, 6 and 7. The karyotype were detected as 46,X,t(X;5)(p22.3;q22) in case 4 and 46,X,der(X)t(X;Y)(p22.3;q11.2) in cases 6 and 7. These patients exhibited unremarkable clinical manifestations but experienced a history of abnormal chromosomal pregnancy. Normal phenotype and a complex reciprocal translocation as 46,X,t(X;14;4)(q24;q22;q33) were observed in case 5 with a history of spontaneous abortions. In the three male patients, multiple semen analyses confirmed the absence of sperm. Y chromosome microdeletion and hormonal analyses were normal. The karyotypes were detected as 46,Y,t(X;8)(q26;q22), 46,Y,t(X;1)(q26;q23), 46,Y,t(X;3)(q26;p24), respectively.</p><p><strong>Conclusions: </strong>Our study provides insights into individuals with X chromosome translocations. The clinical phenotypes are variable and unpredictable due to differences in breakpoints and X chromosome inactivation (XCI) patterns. Our results suggest that physicians should focus on the characteristics of the X chromosome translocations and provide personalized clinical evaluations in genetic counselling.</p>\",\"PeriodicalId\":19099,\"journal\":{\"name\":\"Molecular Cytogenetics\",\"volume\":\"16 1\",\"pages\":\"36\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2023-12-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10740294/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Molecular Cytogenetics\",\"FirstCategoryId\":\"99\",\"ListUrlMain\":\"https://doi.org/10.1186/s13039-023-00669-7\",\"RegionNum\":4,\"RegionCategory\":\"生物学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"GENETICS & HEREDITY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Molecular Cytogenetics","FirstCategoryId":"99","ListUrlMain":"https://doi.org/10.1186/s13039-023-00669-7","RegionNum":4,"RegionCategory":"生物学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GENETICS & HEREDITY","Score":null,"Total":0}
引用次数: 0
摘要
背景:具有 X 染色体易位、多变表型和活产缺陷高风险的个体是科学研究的兴趣所在。这些特征与不同的断点和各种类型的染色体异常有关。为了研究 X 染色体易位对临床表型的影响,我们对 X 染色体易位患者的临床数据进行了回顾性分析。所有患者均进行了核型分析和内分泌评估。此外,还对男性患者的精液分析和 Y 染色体微缺失情况进行了评估:结果:10 例患者中检测到 X 染色体易位,其中女性 7 例,男性 3 例。在病例 1(FSH:114 IU/L,LH:30.90 mIU/mL,E2:结论:我们的研究让我们对 X 染色体易位患者有了更深入的了解。由于断点和 X 染色体失活(XCI)模式的差异,临床表型多变且难以预测。我们的研究结果表明,医生应关注 X 染色体易位的特征,并在遗传咨询中提供个性化的临床评估。
Characteristics and clinical evaluation of X chromosome translocations.
Background: Individuals with X chromosomal translocations, variable phenotypes, and a high risk of live birth defects are of interest for scientific study. These characteristics are related to differential breakpoints and various types of chromosomal abnormalities. To investigate the effects of X chromosome translocation on clinical phenotype, a retrospective analysis of clinical data for patients with X chromosome translocation was conducted. Karyotype analysis plus endocrine evaluation was utilized for all the patients. Additional semen analysis and Y chromosome microdeletions were assessed in male patients.
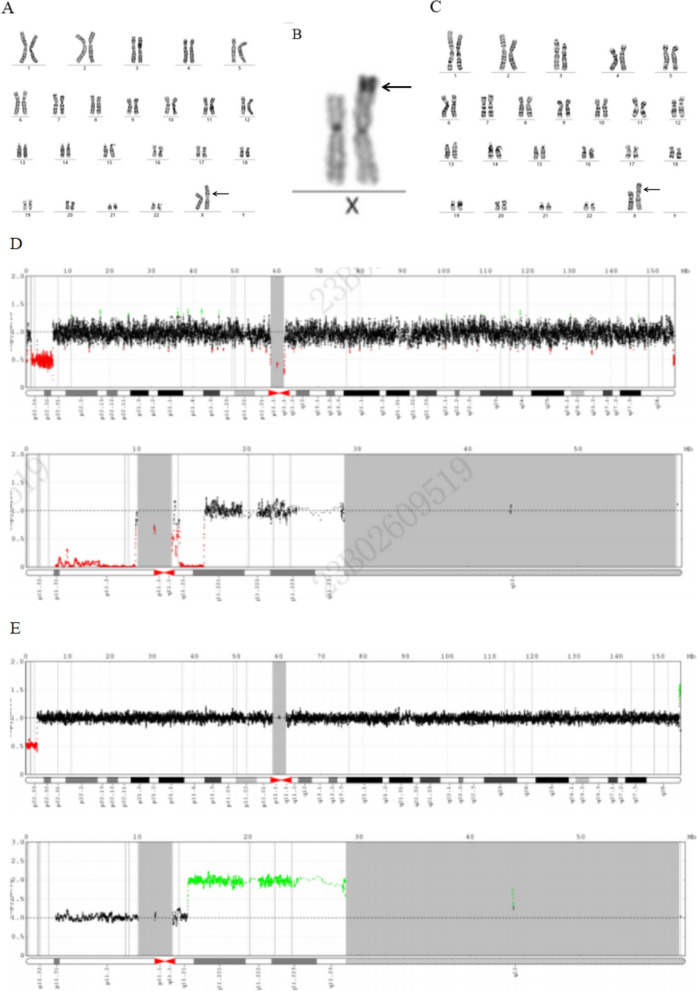
Results: X chromosome translocations were detected in ten cases, including seven females and three males. Infantile uterus and no ovaries were detected in case 1 (FSH: 114 IU/L, LH: 30.90 mIU/mL, E2: < 5.00 pg/ml), and the karyotype was confirmed as 46,X,t(X;22)(q25;q11.2) in case 1. Infantile uterus and small ovaries were both visible in two cases (FSH: 34.80 IU/L, LH: 17.06 mIU/mL, E2: 15.37 pg/ml in case 2; FISH: 6.60 IU/L, LH: 1.69 mIU/mL, E2: 23.70 pg/ml in case 3). The karyotype was detected as 46,X,t(X;8)(q13;q11.2) in case 2 and 46,X,der(X)t(X;5)(q21;q31) in case 3. Normal reproductive hormone levels and fertility abilities were found for cases 4, 6 and 7. The karyotype were detected as 46,X,t(X;5)(p22.3;q22) in case 4 and 46,X,der(X)t(X;Y)(p22.3;q11.2) in cases 6 and 7. These patients exhibited unremarkable clinical manifestations but experienced a history of abnormal chromosomal pregnancy. Normal phenotype and a complex reciprocal translocation as 46,X,t(X;14;4)(q24;q22;q33) were observed in case 5 with a history of spontaneous abortions. In the three male patients, multiple semen analyses confirmed the absence of sperm. Y chromosome microdeletion and hormonal analyses were normal. The karyotypes were detected as 46,Y,t(X;8)(q26;q22), 46,Y,t(X;1)(q26;q23), 46,Y,t(X;3)(q26;p24), respectively.
Conclusions: Our study provides insights into individuals with X chromosome translocations. The clinical phenotypes are variable and unpredictable due to differences in breakpoints and X chromosome inactivation (XCI) patterns. Our results suggest that physicians should focus on the characteristics of the X chromosome translocations and provide personalized clinical evaluations in genetic counselling.
期刊介绍:
Molecular Cytogenetics encompasses all aspects of chromosome biology and the application of molecular cytogenetic techniques in all areas of biology and medicine, including structural and functional organization of the chromosome and nucleus, genome variation, expression and evolution, chromosome abnormalities and genomic variations in medical genetics and tumor genetics.
Molecular Cytogenetics primarily defines a large set of the techniques that operate either with the entire genome or with specific targeted DNA sequences. Topical areas include, but are not limited to:
-Structural and functional organization of chromosome and nucleus-
Genome variation, expression and evolution-
Animal and plant molecular cytogenetics and genomics-
Chromosome abnormalities and genomic variations in clinical genetics-
Applications in preimplantation, pre- and post-natal diagnosis-
Applications in the central nervous system, cancer and haematology research-
Previously unreported applications of molecular cytogenetic techniques-
Development of new techniques or significant enhancements to established techniques.
This journal is a source for numerous scientists all over the world, who wish to improve or introduce molecular cytogenetic techniques into their practice.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


