M. Picardi, C. Giordano, N. Pugliese, M. Mascolo, S. Varricchio, G. Troncone, E. Vigliar, C. Bellavicine, M. Lamagna, D. Lisi, A. Vincenzi, F. Pane
{"title":"脂质体包裹多柔比星增量一线治疗可提高原发性纵隔大B细胞淋巴瘤和纵隔灰区淋巴瘤的应答率","authors":"M. Picardi, C. Giordano, N. Pugliese, M. Mascolo, S. Varricchio, G. Troncone, E. Vigliar, C. Bellavicine, M. Lamagna, D. Lisi, A. Vincenzi, F. Pane","doi":"10.1002/hon.3242","DOIUrl":null,"url":null,"abstract":"<p>Tumor-infiltrating macrophages (TIMs) are constantly ≥5% staining at immunohistochemical analysis on biopsy specimens of tumor masses, in primary mediastinal large B-cell lymphoma (PMBL) and mediastinal gray zone lymphoma (MGZL).<span><sup>1-3</sup></span> The presence of many CD68-positive TIMs into lymph node microenvironment of both PMBL and MGZL is associated with shortened progression-free survival (PFS) following conventional anthracycline-based regimens.<span><sup>1-3</sup></span> Myocet™ is doxorubicin encapsulated in a non-pegylated liposomal membrane of phosphatidylcholine and cholesterol.<span><sup>4</sup></span> Increased dosages of non-pegylated liposomal-encapsulated doxorubicin (NPLD) may have some pharmacokinetic and pharmacodynamic advantages<span><sup>4, 5</sup></span> since it rapidly accumulates at high levels within macrophage cells of the microenvironment of malignant lymphadenopathies, acting as slow-release reservoir with prolonged powerful tumoricidal effects specifically inside the neoplastic tissue.<span><sup>6, 7</sup></span> These effects might be perceived as a great benefit in those patients with aggressive non-Hodgkin lymphoma with high tumor burden. For this reason, a dose intensified (DI) strategy with NPLD was used for untreated advanced-stage diffuse large B-cell lymphoma (DLBCL), instead of hydroxydaunorubicin in rituximab, cyclophosphamide, hydroxydaunorubicin, vincristine and prednisone (R-CHOP), thus constituting a new regimen, so called R-COMP-DI.<span><sup>8</sup></span> The scheme resulted to have better activity profile compared to the historical R-CHOP data.<span><sup>8, 9</sup></span> Furthermore, a personal extrapolation from published data showed very low rate of discontinued treatment due to drug related adverse events following intensified version of R-COMP.<span><sup>8-10</sup></span> On the basis of these data, in our Institution a frontline approach with increased dosage of Myocet™ has been routinely employed in PMBL and MGZL for the last 6 years. We report a real-life experience on the efficacy and safety of a new scheme named R-COMP-DI<sup>x6</sup>, with a supercharge dose of NPLD for six cycles every 3 weeks, in patients with newly diagnosed PMBL and MGZL. The R-COMP-DI<sup>x6</sup> schedule consisted of 1-day outpatient intravenous infusions of Myocet™ at an escalated dose of 70 mg/m<sup>2</sup>, plus rituximab 375 mg/m<sup>2</sup>, cyclophosphamide 750 mg/m<sup>2</sup>, vincristine 1.4 mg/m<sup>2</sup> (up to a maximal dose of 2 mg) and prednisone 40 mg/m<sup>2</sup> per day for 5 days, at a 3-week interval for a total of six cycles. The cumulative dose of NPLD was 420 mg/m<sup>2</sup> for the entire scheme of 6 cycles giving an increased dose of 70 mg/m<sup>2</sup> per each cycle. The dose-intensity of NPLD in cycles one to six of R-COMP-DI<sup>x6</sup> was increased to 140% of standard dosage and was well within the ceiling dose of 785 mg/m<sup>2</sup> (the median lifetime dose reported for NPLD at the onset of cardiotoxicity).<span><sup>4, 5</sup></span> Noteworthy, in our study the cardiologic toxicity profile was established by using the echocardiography assessment of global systolic longitudinal myocardial strain (GLS), as well as left ventricular ejection fraction (LVEF), according to the guidelines of the Task Force for Cancer Treatments and Cardiovascular Toxicity of the European Society of Cardiology.<span><sup>11</sup></span></p><p>The primary endpoint was the activity of the liposomal doxorubicin supercharge-based front-line strategy in terms of end-of-treatment (EoT) 2-deoxy-2[F-18] fluoro-D-glucose positron emission tomography (FDG-PET) negativity (as already described).<span><sup>12-14</sup></span> Secondary endpoints were toxicity (according to the National Cancer Institute Common Terminology Criteria for Adverse Events version 5.0) and PFS (defined as the time from day 1 of R-COMP-DI<sup>x6</sup> first dose to disease progression/relapse [event], death from any cause [event] or last follow-up visit [censoring]). Finally, CD68 stains were scored as 1+ (5%–25% positive cells observed), 2+ (26%–50%) and 3+ (>50%) at lymph node microenvironment immunohistochemistry as already reported<span><sup>1-3</sup></span>; the optimum cutoff point which correlated with better outcome following R-COMP-DI<sup>x6</sup> was explored according to the proposed macrophage's stain score.</p><p>The study was conducted in the Hematology Unit of the Federico II University of Naples (Italy) and was undertaken in accordance with the Declaration of Helsinki. All necessary approvals were obtained from our ethics committee. A dedicated written informed consent form for intensive immunochemotherapy treatment was obtained from each patient before therapy start. Consecutive patients with previously untreated, biopsy confirmed PMBL and MGZL<span><sup>15</sup></span> receiving front-line therapy from 1 March 2016 to 31 January 2022, were retrospectively screened. All patients receiving the high-dosage Myocet™-based scheme, that is, R-COMP-DI<sup>x6</sup>, with ≥18 and ≤60 years, Ann Arbor Stage I-IV, Eastern Cooperative Group Performance Status 0–2, GLS≥ −20% at baseline echocardiography assessment, and availability of pathological lymph node samples obtained by surgical biopsy routinely fixed in formalin and embedded in paraffin (histological sections stained with haematoxylin and eosin, and Giemsa) reporting morphological and immunohistochemical features (either reported on the original report or, whenever this was missing, as assessed retrospectively by at least three expert haematopathologists with >10 years of experience with haematopathological evaluations) were finally included in the analysis. Vigorous support drug treatment and clinical/laboratory/imaging monitoring were systematically performed in all patients, as already described.<span><sup>8</sup></span> Patients routinely underwent a full cardiologic examination, two-dimensional echocardiography, and speckle tracking echocardiography at baseline, interim, EoT and within 6 months from the end of all antineoplastic treatments, as already reported.<span><sup>16</sup></span></p><p>Table 1 shows the clinical characteristics of all patients enrolled (<i>n</i> = 14). The median age was 42 years (range, 24–60 years), and the 57% were female. The 71% of cases had Ann Arbor stage I to II. The 86% of patients had a mediastinal nodal mass larger than 7 cm (median, 9 cm; range, 7.5–13 cm), and the 50% had elevated serum lactate dehydrogenase. Six patients had unfavorable international prognostic index. Nine cases had histologic and phenotypic features of PMBL, and the remaining five had histologic and phenotypic features of MGZL. The expert haematopathologists confirmed the diagnoses according to the World Health Organization of Tumors of Haematopoietic and Lymphoid Tissues.<span><sup>15</sup></span> Regarding the dose-intensity of the planned treatment, 12 patients received full dose (100%), and two patients (PMBL) received a dose-intensity between 85% and 99%. The median (range) duration of R-COMP-DI<sup>x6</sup> was 126 (126–155) days as the expected duration of 126 days. All patients were assessable for the final responses after R-COMP-DI<sup>x6</sup> regimen. FDG-PET scans were performed between 5 and 6 weeks (median, 5) after the sixth immunochemotherapy cycle. Thirteen of the 14 patients had negative EoT-PET scans, reaching the complete metabolic response (CMR). Thus, the primary endpoint of the study in terms of complete response incidence at EoT-imaging assessment, that is, CMR rate, was 92.8% (95% CI, 0.5%–1.58%). In detail, among the nine patients with PMBL who completed six R-COMP intensified cycles, only one (11%) had positive EoT-PET scans; and, among the five patients with MGZL, none had a positive EoT-PET. The analysis of post-R-COMP-DI<sup>x6</sup> imaging scans assigned a Deauville score (DS) as follows: DS 1 to four patients, DS 2 to five patients, DS 3 to four patients, and DS 5 to one patient. The response data based on the percentage change in tumor volume from baseline as evaluated by morphologic imaging (<i>i.e.</i>, computed tomography scans) showed a 100% decrease in lymph node size for each patient, except for three cases with residual tissue (<i>i.e.</i>, nodes >2 cm long axis) in the initial mediastinal large nodal mass site. No patient received consolidation radiotherapy (c-RT); the patient with PMBL with EoT-PET with DS 5 received salvage therapy and autologous hematopoietic stem cell transplantation. A complete echocardiography evaluation (including measurements of GLS and LVEF, and performed at baseline, interim, EoT and 6 months later) was available for 13 patients. There were very small changes in three patients, that is, <10% point reductions in values of GLS (and <5% point reductions in values of LVEF) at interim, EoT and/or 6-month follow-up, when the measurements were compared with the values at baseline (GLS of −21%, LVEF of >50%). Regarding hematological toxicity, two patients reported anemia of Grade 3; and three patients reported at least one neutropenic event of Grade 3. Two patients reported Grade 3 gastrointestinal toxicity events (one, diarrhea; one, paralytic ileum). None of the patients required hospitalization to manage treatment-related adverse events. At a median (range) follow-up of 24 (1–55) months, for the entire cohort of 14 patients, the PFS was 92.8% (95% CI, 52%–98%) (Figure 1). The analysis of CD68 stains at lymph node microenvironment immunohistochemistry showed that, with a subgrouping in 1+ (<i>n</i> = 3) versus 2+ to 3+ (<i>n</i> = 11) scores, the 2-year PFS was 66% and 100% respectively (<i>p</i> = 0.05). This suggests a trend that many tumor-associated macrophages (cutoff point, >25%) had a favorable prognostic impact when R-COMP-DI<sup>x6</sup> regimen was administered in both PMBL and MGZL (Figure 1). Because of the limited number of patients, these results need to be assessed in a larger series.</p><p>PMBL and MGZL are characterized by poor prognosis when adequate responses are not rapidly achieved or if the disease recurs.<span><sup>1, 3, 17</sup></span> In these patients at high risk, individualized dose escalation is predicted to be most effective when applied during the upfront therapy. The superiority over the standard R-CHOP-21 of dose-intensive immuno-chemotherapy regimens has not been proven by randomized trials. The IELSG 37 study on a large series of patients (<i>n</i> = 505) has shown that patients treated with dose intensive regimens as R-CHOP-14, R-MACOP-B and DA-EPOCH-R had better EOT responses (DS ≤ 3) when compared with R-CHOP-21.<span><sup>17</sup></span> However, these regimens come with not negligible associated toxicities.<span><sup>1, 3, 17</sup></span> c-RT can consolidate responses after induction, but it may increase the risk of second malignancies and accelerate coronary heart disease. Our retrospective study shows the efficacy of liposomal doxorubicin supercharge-based front-line therapy in both PMBL and MGZL, as reflected by a substantial increase in the number of patients with EoT-FDG-PET negativity. In the PMBL subgroup, the negative EoT-FDG-PET scans rate following the six scheduled R-COMP-DI cycles was 89% versus 55% of the pooled summary negativity EoT-PET rate of the literature following R-CHOP-21 in a similar patient setting.<span><sup>9, 17</sup></span> The rate of the negative EoT-FDG-PET scans following the six scheduled R-COMP-DI cycles in the MGZL sub-group was 100% versus 58% of the pooled summary EoT-FDG-PET negativity rate of the literature following conventional anthracycline-based regimens in a similar patient setting.<span><sup>1, 3</sup></span> We perceived these results with high clinical interest for the absolute improvement of ≥34% points of EoT-FDG-PET with negative findings in both lymphoma sub-types following NPLD high-dose-containing upfront treatment. However, we admit that the comparison with the published standard approaches was approximate from personal extrapolations of the authors based on the features available in each report.<span><sup>1, 3, 9, 17</sup></span> In addition, the study presents two major limits: the small number of total patients enrolled (<i>n</i> = 14), of which 9 PMBCLs and 5 MGZLs, and a long time of accrual (about 6 years) that may lead to a high selection patient's bias.</p><p>In conclusion, this single-center, non-controlled, small study conducted retrospectively in a high-risk setting of adult (age ≤60 years) patients with PMBL or MGZL suggests that frontline treatment with R-COMP-DI<sup>x6</sup>, including increasing dosages of liposomal doxorubicin, is a ‘proof of concept’ for testing it in a large multicenter phase II clinical trial.</p><p>Authors have no relevant financial conflict of interest to declare.</p>","PeriodicalId":12882,"journal":{"name":"Hematological Oncology","volume":"42 1","pages":""},"PeriodicalIF":3.3000,"publicationDate":"2023-12-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/hon.3242","citationCount":"0","resultStr":"{\"title\":\"Liposomal-encapsulated doxorubicin supercharge-containing front-line treatment improves response rates in primary mediastinal large B-cell lymphoma and mediastinal gray zone lymphoma\",\"authors\":\"M. Picardi, C. Giordano, N. Pugliese, M. Mascolo, S. Varricchio, G. Troncone, E. Vigliar, C. Bellavicine, M. Lamagna, D. Lisi, A. Vincenzi, F. Pane\",\"doi\":\"10.1002/hon.3242\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Tumor-infiltrating macrophages (TIMs) are constantly ≥5% staining at immunohistochemical analysis on biopsy specimens of tumor masses, in primary mediastinal large B-cell lymphoma (PMBL) and mediastinal gray zone lymphoma (MGZL).<span><sup>1-3</sup></span> The presence of many CD68-positive TIMs into lymph node microenvironment of both PMBL and MGZL is associated with shortened progression-free survival (PFS) following conventional anthracycline-based regimens.<span><sup>1-3</sup></span> Myocet™ is doxorubicin encapsulated in a non-pegylated liposomal membrane of phosphatidylcholine and cholesterol.<span><sup>4</sup></span> Increased dosages of non-pegylated liposomal-encapsulated doxorubicin (NPLD) may have some pharmacokinetic and pharmacodynamic advantages<span><sup>4, 5</sup></span> since it rapidly accumulates at high levels within macrophage cells of the microenvironment of malignant lymphadenopathies, acting as slow-release reservoir with prolonged powerful tumoricidal effects specifically inside the neoplastic tissue.<span><sup>6, 7</sup></span> These effects might be perceived as a great benefit in those patients with aggressive non-Hodgkin lymphoma with high tumor burden. For this reason, a dose intensified (DI) strategy with NPLD was used for untreated advanced-stage diffuse large B-cell lymphoma (DLBCL), instead of hydroxydaunorubicin in rituximab, cyclophosphamide, hydroxydaunorubicin, vincristine and prednisone (R-CHOP), thus constituting a new regimen, so called R-COMP-DI.<span><sup>8</sup></span> The scheme resulted to have better activity profile compared to the historical R-CHOP data.<span><sup>8, 9</sup></span> Furthermore, a personal extrapolation from published data showed very low rate of discontinued treatment due to drug related adverse events following intensified version of R-COMP.<span><sup>8-10</sup></span> On the basis of these data, in our Institution a frontline approach with increased dosage of Myocet™ has been routinely employed in PMBL and MGZL for the last 6 years. We report a real-life experience on the efficacy and safety of a new scheme named R-COMP-DI<sup>x6</sup>, with a supercharge dose of NPLD for six cycles every 3 weeks, in patients with newly diagnosed PMBL and MGZL. The R-COMP-DI<sup>x6</sup> schedule consisted of 1-day outpatient intravenous infusions of Myocet™ at an escalated dose of 70 mg/m<sup>2</sup>, plus rituximab 375 mg/m<sup>2</sup>, cyclophosphamide 750 mg/m<sup>2</sup>, vincristine 1.4 mg/m<sup>2</sup> (up to a maximal dose of 2 mg) and prednisone 40 mg/m<sup>2</sup> per day for 5 days, at a 3-week interval for a total of six cycles. The cumulative dose of NPLD was 420 mg/m<sup>2</sup> for the entire scheme of 6 cycles giving an increased dose of 70 mg/m<sup>2</sup> per each cycle. The dose-intensity of NPLD in cycles one to six of R-COMP-DI<sup>x6</sup> was increased to 140% of standard dosage and was well within the ceiling dose of 785 mg/m<sup>2</sup> (the median lifetime dose reported for NPLD at the onset of cardiotoxicity).<span><sup>4, 5</sup></span> Noteworthy, in our study the cardiologic toxicity profile was established by using the echocardiography assessment of global systolic longitudinal myocardial strain (GLS), as well as left ventricular ejection fraction (LVEF), according to the guidelines of the Task Force for Cancer Treatments and Cardiovascular Toxicity of the European Society of Cardiology.<span><sup>11</sup></span></p><p>The primary endpoint was the activity of the liposomal doxorubicin supercharge-based front-line strategy in terms of end-of-treatment (EoT) 2-deoxy-2[F-18] fluoro-D-glucose positron emission tomography (FDG-PET) negativity (as already described).<span><sup>12-14</sup></span> Secondary endpoints were toxicity (according to the National Cancer Institute Common Terminology Criteria for Adverse Events version 5.0) and PFS (defined as the time from day 1 of R-COMP-DI<sup>x6</sup> first dose to disease progression/relapse [event], death from any cause [event] or last follow-up visit [censoring]). Finally, CD68 stains were scored as 1+ (5%–25% positive cells observed), 2+ (26%–50%) and 3+ (>50%) at lymph node microenvironment immunohistochemistry as already reported<span><sup>1-3</sup></span>; the optimum cutoff point which correlated with better outcome following R-COMP-DI<sup>x6</sup> was explored according to the proposed macrophage's stain score.</p><p>The study was conducted in the Hematology Unit of the Federico II University of Naples (Italy) and was undertaken in accordance with the Declaration of Helsinki. All necessary approvals were obtained from our ethics committee. A dedicated written informed consent form for intensive immunochemotherapy treatment was obtained from each patient before therapy start. Consecutive patients with previously untreated, biopsy confirmed PMBL and MGZL<span><sup>15</sup></span> receiving front-line therapy from 1 March 2016 to 31 January 2022, were retrospectively screened. All patients receiving the high-dosage Myocet™-based scheme, that is, R-COMP-DI<sup>x6</sup>, with ≥18 and ≤60 years, Ann Arbor Stage I-IV, Eastern Cooperative Group Performance Status 0–2, GLS≥ −20% at baseline echocardiography assessment, and availability of pathological lymph node samples obtained by surgical biopsy routinely fixed in formalin and embedded in paraffin (histological sections stained with haematoxylin and eosin, and Giemsa) reporting morphological and immunohistochemical features (either reported on the original report or, whenever this was missing, as assessed retrospectively by at least three expert haematopathologists with >10 years of experience with haematopathological evaluations) were finally included in the analysis. Vigorous support drug treatment and clinical/laboratory/imaging monitoring were systematically performed in all patients, as already described.<span><sup>8</sup></span> Patients routinely underwent a full cardiologic examination, two-dimensional echocardiography, and speckle tracking echocardiography at baseline, interim, EoT and within 6 months from the end of all antineoplastic treatments, as already reported.<span><sup>16</sup></span></p><p>Table 1 shows the clinical characteristics of all patients enrolled (<i>n</i> = 14). The median age was 42 years (range, 24–60 years), and the 57% were female. The 71% of cases had Ann Arbor stage I to II. The 86% of patients had a mediastinal nodal mass larger than 7 cm (median, 9 cm; range, 7.5–13 cm), and the 50% had elevated serum lactate dehydrogenase. Six patients had unfavorable international prognostic index. Nine cases had histologic and phenotypic features of PMBL, and the remaining five had histologic and phenotypic features of MGZL. The expert haematopathologists confirmed the diagnoses according to the World Health Organization of Tumors of Haematopoietic and Lymphoid Tissues.<span><sup>15</sup></span> Regarding the dose-intensity of the planned treatment, 12 patients received full dose (100%), and two patients (PMBL) received a dose-intensity between 85% and 99%. The median (range) duration of R-COMP-DI<sup>x6</sup> was 126 (126–155) days as the expected duration of 126 days. All patients were assessable for the final responses after R-COMP-DI<sup>x6</sup> regimen. FDG-PET scans were performed between 5 and 6 weeks (median, 5) after the sixth immunochemotherapy cycle. Thirteen of the 14 patients had negative EoT-PET scans, reaching the complete metabolic response (CMR). Thus, the primary endpoint of the study in terms of complete response incidence at EoT-imaging assessment, that is, CMR rate, was 92.8% (95% CI, 0.5%–1.58%). In detail, among the nine patients with PMBL who completed six R-COMP intensified cycles, only one (11%) had positive EoT-PET scans; and, among the five patients with MGZL, none had a positive EoT-PET. The analysis of post-R-COMP-DI<sup>x6</sup> imaging scans assigned a Deauville score (DS) as follows: DS 1 to four patients, DS 2 to five patients, DS 3 to four patients, and DS 5 to one patient. The response data based on the percentage change in tumor volume from baseline as evaluated by morphologic imaging (<i>i.e.</i>, computed tomography scans) showed a 100% decrease in lymph node size for each patient, except for three cases with residual tissue (<i>i.e.</i>, nodes >2 cm long axis) in the initial mediastinal large nodal mass site. No patient received consolidation radiotherapy (c-RT); the patient with PMBL with EoT-PET with DS 5 received salvage therapy and autologous hematopoietic stem cell transplantation. A complete echocardiography evaluation (including measurements of GLS and LVEF, and performed at baseline, interim, EoT and 6 months later) was available for 13 patients. There were very small changes in three patients, that is, <10% point reductions in values of GLS (and <5% point reductions in values of LVEF) at interim, EoT and/or 6-month follow-up, when the measurements were compared with the values at baseline (GLS of −21%, LVEF of >50%). Regarding hematological toxicity, two patients reported anemia of Grade 3; and three patients reported at least one neutropenic event of Grade 3. Two patients reported Grade 3 gastrointestinal toxicity events (one, diarrhea; one, paralytic ileum). None of the patients required hospitalization to manage treatment-related adverse events. At a median (range) follow-up of 24 (1–55) months, for the entire cohort of 14 patients, the PFS was 92.8% (95% CI, 52%–98%) (Figure 1). The analysis of CD68 stains at lymph node microenvironment immunohistochemistry showed that, with a subgrouping in 1+ (<i>n</i> = 3) versus 2+ to 3+ (<i>n</i> = 11) scores, the 2-year PFS was 66% and 100% respectively (<i>p</i> = 0.05). This suggests a trend that many tumor-associated macrophages (cutoff point, >25%) had a favorable prognostic impact when R-COMP-DI<sup>x6</sup> regimen was administered in both PMBL and MGZL (Figure 1). Because of the limited number of patients, these results need to be assessed in a larger series.</p><p>PMBL and MGZL are characterized by poor prognosis when adequate responses are not rapidly achieved or if the disease recurs.<span><sup>1, 3, 17</sup></span> In these patients at high risk, individualized dose escalation is predicted to be most effective when applied during the upfront therapy. The superiority over the standard R-CHOP-21 of dose-intensive immuno-chemotherapy regimens has not been proven by randomized trials. The IELSG 37 study on a large series of patients (<i>n</i> = 505) has shown that patients treated with dose intensive regimens as R-CHOP-14, R-MACOP-B and DA-EPOCH-R had better EOT responses (DS ≤ 3) when compared with R-CHOP-21.<span><sup>17</sup></span> However, these regimens come with not negligible associated toxicities.<span><sup>1, 3, 17</sup></span> c-RT can consolidate responses after induction, but it may increase the risk of second malignancies and accelerate coronary heart disease. Our retrospective study shows the efficacy of liposomal doxorubicin supercharge-based front-line therapy in both PMBL and MGZL, as reflected by a substantial increase in the number of patients with EoT-FDG-PET negativity. In the PMBL subgroup, the negative EoT-FDG-PET scans rate following the six scheduled R-COMP-DI cycles was 89% versus 55% of the pooled summary negativity EoT-PET rate of the literature following R-CHOP-21 in a similar patient setting.<span><sup>9, 17</sup></span> The rate of the negative EoT-FDG-PET scans following the six scheduled R-COMP-DI cycles in the MGZL sub-group was 100% versus 58% of the pooled summary EoT-FDG-PET negativity rate of the literature following conventional anthracycline-based regimens in a similar patient setting.<span><sup>1, 3</sup></span> We perceived these results with high clinical interest for the absolute improvement of ≥34% points of EoT-FDG-PET with negative findings in both lymphoma sub-types following NPLD high-dose-containing upfront treatment. However, we admit that the comparison with the published standard approaches was approximate from personal extrapolations of the authors based on the features available in each report.<span><sup>1, 3, 9, 17</sup></span> In addition, the study presents two major limits: the small number of total patients enrolled (<i>n</i> = 14), of which 9 PMBCLs and 5 MGZLs, and a long time of accrual (about 6 years) that may lead to a high selection patient's bias.</p><p>In conclusion, this single-center, non-controlled, small study conducted retrospectively in a high-risk setting of adult (age ≤60 years) patients with PMBL or MGZL suggests that frontline treatment with R-COMP-DI<sup>x6</sup>, including increasing dosages of liposomal doxorubicin, is a ‘proof of concept’ for testing it in a large multicenter phase II clinical trial.</p><p>Authors have no relevant financial conflict of interest to declare.</p>\",\"PeriodicalId\":12882,\"journal\":{\"name\":\"Hematological Oncology\",\"volume\":\"42 1\",\"pages\":\"\"},\"PeriodicalIF\":3.3000,\"publicationDate\":\"2023-12-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/hon.3242\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Hematological Oncology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/hon.3242\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Hematological Oncology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/hon.3242","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEMATOLOGY","Score":null,"Total":0}
Liposomal-encapsulated doxorubicin supercharge-containing front-line treatment improves response rates in primary mediastinal large B-cell lymphoma and mediastinal gray zone lymphoma
Tumor-infiltrating macrophages (TIMs) are constantly ≥5% staining at immunohistochemical analysis on biopsy specimens of tumor masses, in primary mediastinal large B-cell lymphoma (PMBL) and mediastinal gray zone lymphoma (MGZL).1-3 The presence of many CD68-positive TIMs into lymph node microenvironment of both PMBL and MGZL is associated with shortened progression-free survival (PFS) following conventional anthracycline-based regimens.1-3 Myocet™ is doxorubicin encapsulated in a non-pegylated liposomal membrane of phosphatidylcholine and cholesterol.4 Increased dosages of non-pegylated liposomal-encapsulated doxorubicin (NPLD) may have some pharmacokinetic and pharmacodynamic advantages4, 5 since it rapidly accumulates at high levels within macrophage cells of the microenvironment of malignant lymphadenopathies, acting as slow-release reservoir with prolonged powerful tumoricidal effects specifically inside the neoplastic tissue.6, 7 These effects might be perceived as a great benefit in those patients with aggressive non-Hodgkin lymphoma with high tumor burden. For this reason, a dose intensified (DI) strategy with NPLD was used for untreated advanced-stage diffuse large B-cell lymphoma (DLBCL), instead of hydroxydaunorubicin in rituximab, cyclophosphamide, hydroxydaunorubicin, vincristine and prednisone (R-CHOP), thus constituting a new regimen, so called R-COMP-DI.8 The scheme resulted to have better activity profile compared to the historical R-CHOP data.8, 9 Furthermore, a personal extrapolation from published data showed very low rate of discontinued treatment due to drug related adverse events following intensified version of R-COMP.8-10 On the basis of these data, in our Institution a frontline approach with increased dosage of Myocet™ has been routinely employed in PMBL and MGZL for the last 6 years. We report a real-life experience on the efficacy and safety of a new scheme named R-COMP-DIx6, with a supercharge dose of NPLD for six cycles every 3 weeks, in patients with newly diagnosed PMBL and MGZL. The R-COMP-DIx6 schedule consisted of 1-day outpatient intravenous infusions of Myocet™ at an escalated dose of 70 mg/m2, plus rituximab 375 mg/m2, cyclophosphamide 750 mg/m2, vincristine 1.4 mg/m2 (up to a maximal dose of 2 mg) and prednisone 40 mg/m2 per day for 5 days, at a 3-week interval for a total of six cycles. The cumulative dose of NPLD was 420 mg/m2 for the entire scheme of 6 cycles giving an increased dose of 70 mg/m2 per each cycle. The dose-intensity of NPLD in cycles one to six of R-COMP-DIx6 was increased to 140% of standard dosage and was well within the ceiling dose of 785 mg/m2 (the median lifetime dose reported for NPLD at the onset of cardiotoxicity).4, 5 Noteworthy, in our study the cardiologic toxicity profile was established by using the echocardiography assessment of global systolic longitudinal myocardial strain (GLS), as well as left ventricular ejection fraction (LVEF), according to the guidelines of the Task Force for Cancer Treatments and Cardiovascular Toxicity of the European Society of Cardiology.11
The primary endpoint was the activity of the liposomal doxorubicin supercharge-based front-line strategy in terms of end-of-treatment (EoT) 2-deoxy-2[F-18] fluoro-D-glucose positron emission tomography (FDG-PET) negativity (as already described).12-14 Secondary endpoints were toxicity (according to the National Cancer Institute Common Terminology Criteria for Adverse Events version 5.0) and PFS (defined as the time from day 1 of R-COMP-DIx6 first dose to disease progression/relapse [event], death from any cause [event] or last follow-up visit [censoring]). Finally, CD68 stains were scored as 1+ (5%–25% positive cells observed), 2+ (26%–50%) and 3+ (>50%) at lymph node microenvironment immunohistochemistry as already reported1-3; the optimum cutoff point which correlated with better outcome following R-COMP-DIx6 was explored according to the proposed macrophage's stain score.
The study was conducted in the Hematology Unit of the Federico II University of Naples (Italy) and was undertaken in accordance with the Declaration of Helsinki. All necessary approvals were obtained from our ethics committee. A dedicated written informed consent form for intensive immunochemotherapy treatment was obtained from each patient before therapy start. Consecutive patients with previously untreated, biopsy confirmed PMBL and MGZL15 receiving front-line therapy from 1 March 2016 to 31 January 2022, were retrospectively screened. All patients receiving the high-dosage Myocet™-based scheme, that is, R-COMP-DIx6, with ≥18 and ≤60 years, Ann Arbor Stage I-IV, Eastern Cooperative Group Performance Status 0–2, GLS≥ −20% at baseline echocardiography assessment, and availability of pathological lymph node samples obtained by surgical biopsy routinely fixed in formalin and embedded in paraffin (histological sections stained with haematoxylin and eosin, and Giemsa) reporting morphological and immunohistochemical features (either reported on the original report or, whenever this was missing, as assessed retrospectively by at least three expert haematopathologists with >10 years of experience with haematopathological evaluations) were finally included in the analysis. Vigorous support drug treatment and clinical/laboratory/imaging monitoring were systematically performed in all patients, as already described.8 Patients routinely underwent a full cardiologic examination, two-dimensional echocardiography, and speckle tracking echocardiography at baseline, interim, EoT and within 6 months from the end of all antineoplastic treatments, as already reported.16
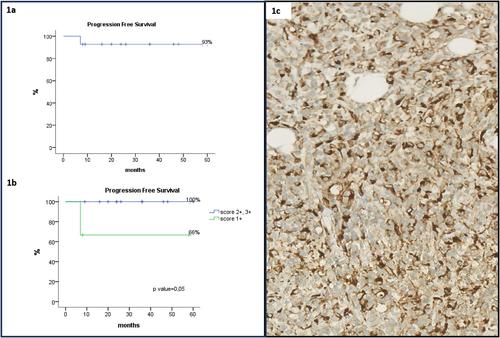
Table 1 shows the clinical characteristics of all patients enrolled (n = 14). The median age was 42 years (range, 24–60 years), and the 57% were female. The 71% of cases had Ann Arbor stage I to II. The 86% of patients had a mediastinal nodal mass larger than 7 cm (median, 9 cm; range, 7.5–13 cm), and the 50% had elevated serum lactate dehydrogenase. Six patients had unfavorable international prognostic index. Nine cases had histologic and phenotypic features of PMBL, and the remaining five had histologic and phenotypic features of MGZL. The expert haematopathologists confirmed the diagnoses according to the World Health Organization of Tumors of Haematopoietic and Lymphoid Tissues.15 Regarding the dose-intensity of the planned treatment, 12 patients received full dose (100%), and two patients (PMBL) received a dose-intensity between 85% and 99%. The median (range) duration of R-COMP-DIx6 was 126 (126–155) days as the expected duration of 126 days. All patients were assessable for the final responses after R-COMP-DIx6 regimen. FDG-PET scans were performed between 5 and 6 weeks (median, 5) after the sixth immunochemotherapy cycle. Thirteen of the 14 patients had negative EoT-PET scans, reaching the complete metabolic response (CMR). Thus, the primary endpoint of the study in terms of complete response incidence at EoT-imaging assessment, that is, CMR rate, was 92.8% (95% CI, 0.5%–1.58%). In detail, among the nine patients with PMBL who completed six R-COMP intensified cycles, only one (11%) had positive EoT-PET scans; and, among the five patients with MGZL, none had a positive EoT-PET. The analysis of post-R-COMP-DIx6 imaging scans assigned a Deauville score (DS) as follows: DS 1 to four patients, DS 2 to five patients, DS 3 to four patients, and DS 5 to one patient. The response data based on the percentage change in tumor volume from baseline as evaluated by morphologic imaging (i.e., computed tomography scans) showed a 100% decrease in lymph node size for each patient, except for three cases with residual tissue (i.e., nodes >2 cm long axis) in the initial mediastinal large nodal mass site. No patient received consolidation radiotherapy (c-RT); the patient with PMBL with EoT-PET with DS 5 received salvage therapy and autologous hematopoietic stem cell transplantation. A complete echocardiography evaluation (including measurements of GLS and LVEF, and performed at baseline, interim, EoT and 6 months later) was available for 13 patients. There were very small changes in three patients, that is, <10% point reductions in values of GLS (and <5% point reductions in values of LVEF) at interim, EoT and/or 6-month follow-up, when the measurements were compared with the values at baseline (GLS of −21%, LVEF of >50%). Regarding hematological toxicity, two patients reported anemia of Grade 3; and three patients reported at least one neutropenic event of Grade 3. Two patients reported Grade 3 gastrointestinal toxicity events (one, diarrhea; one, paralytic ileum). None of the patients required hospitalization to manage treatment-related adverse events. At a median (range) follow-up of 24 (1–55) months, for the entire cohort of 14 patients, the PFS was 92.8% (95% CI, 52%–98%) (Figure 1). The analysis of CD68 stains at lymph node microenvironment immunohistochemistry showed that, with a subgrouping in 1+ (n = 3) versus 2+ to 3+ (n = 11) scores, the 2-year PFS was 66% and 100% respectively (p = 0.05). This suggests a trend that many tumor-associated macrophages (cutoff point, >25%) had a favorable prognostic impact when R-COMP-DIx6 regimen was administered in both PMBL and MGZL (Figure 1). Because of the limited number of patients, these results need to be assessed in a larger series.
PMBL and MGZL are characterized by poor prognosis when adequate responses are not rapidly achieved or if the disease recurs.1, 3, 17 In these patients at high risk, individualized dose escalation is predicted to be most effective when applied during the upfront therapy. The superiority over the standard R-CHOP-21 of dose-intensive immuno-chemotherapy regimens has not been proven by randomized trials. The IELSG 37 study on a large series of patients (n = 505) has shown that patients treated with dose intensive regimens as R-CHOP-14, R-MACOP-B and DA-EPOCH-R had better EOT responses (DS ≤ 3) when compared with R-CHOP-21.17 However, these regimens come with not negligible associated toxicities.1, 3, 17 c-RT can consolidate responses after induction, but it may increase the risk of second malignancies and accelerate coronary heart disease. Our retrospective study shows the efficacy of liposomal doxorubicin supercharge-based front-line therapy in both PMBL and MGZL, as reflected by a substantial increase in the number of patients with EoT-FDG-PET negativity. In the PMBL subgroup, the negative EoT-FDG-PET scans rate following the six scheduled R-COMP-DI cycles was 89% versus 55% of the pooled summary negativity EoT-PET rate of the literature following R-CHOP-21 in a similar patient setting.9, 17 The rate of the negative EoT-FDG-PET scans following the six scheduled R-COMP-DI cycles in the MGZL sub-group was 100% versus 58% of the pooled summary EoT-FDG-PET negativity rate of the literature following conventional anthracycline-based regimens in a similar patient setting.1, 3 We perceived these results with high clinical interest for the absolute improvement of ≥34% points of EoT-FDG-PET with negative findings in both lymphoma sub-types following NPLD high-dose-containing upfront treatment. However, we admit that the comparison with the published standard approaches was approximate from personal extrapolations of the authors based on the features available in each report.1, 3, 9, 17 In addition, the study presents two major limits: the small number of total patients enrolled (n = 14), of which 9 PMBCLs and 5 MGZLs, and a long time of accrual (about 6 years) that may lead to a high selection patient's bias.
In conclusion, this single-center, non-controlled, small study conducted retrospectively in a high-risk setting of adult (age ≤60 years) patients with PMBL or MGZL suggests that frontline treatment with R-COMP-DIx6, including increasing dosages of liposomal doxorubicin, is a ‘proof of concept’ for testing it in a large multicenter phase II clinical trial.
Authors have no relevant financial conflict of interest to declare.
期刊介绍:
Hematological Oncology considers for publication articles dealing with experimental and clinical aspects of neoplastic diseases of the hemopoietic and lymphoid systems and relevant related matters. Translational studies applying basic science to clinical issues are particularly welcomed. Manuscripts dealing with the following areas are encouraged:
-Clinical practice and management of hematological neoplasia, including: acute and chronic leukemias, malignant lymphomas, myeloproliferative disorders
-Diagnostic investigations, including imaging and laboratory assays
-Epidemiology, pathology and pathobiology of hematological neoplasia of hematological diseases
-Therapeutic issues including Phase 1, 2 or 3 trials as well as allogeneic and autologous stem cell transplantation studies
-Aspects of the cell biology, molecular biology, molecular genetics and cytogenetics of normal or diseased hematopoeisis and lymphopoiesis, including stem cells and cytokines and other regulatory systems.
Concise, topical review material is welcomed, especially if it makes new concepts and ideas accessible to a wider community. Proposals for review material may be discussed with the Editor-in-Chief. Collections of case material and case reports will be considered only if they have broader scientific or clinical relevance.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


