{"title":"口服西他沙星导致的心搏骤停","authors":"Yugo Wakayama, Satoshi Yoshimura, Katsuyuki Hanabusa, Nobuhiro Ikeda, Nobuhiro Miyamae, Yasuyuki Sumida","doi":"10.1002/ams2.910","DOIUrl":null,"url":null,"abstract":"<p>A woman aged in her 80s had multiple comorbidities with congestive heart failure, aortic stenosis, and chronic renal failure. The QTc interval 6 months before admission was normal (454 ms) (Figure 1A). Three days pre-admission, the maximum dose of sitafloxacin was prescribed to treat urinary tract infections. She presented with convulsions, a complete atrioventricular block, a prolonged QTc interval (538 ms) (Figure 1B), and recurrent torsade de pointes (TdP) (Figure 1C). Treatment involved 2 g magnesium sulfate infusion, noninvasive positive pressure ventilation, and emergency pacing. After the heart failure management with discontinuation of sitafloxacin, the QTc interval was improved by 501 and 466 ms on day 7 and 20, respectively (Figure 1D,E). She remained healthy at 6-month follow-up. Oral quinolones are commonly prescribed antibiotics in clinical settings<span><sup>1</sup></span>; it could induce QT prolongation as <i>hERG</i> gene class effects on potassium channels and causes TdP, especially in the elderly.<span><sup>1</sup></span> Treatments are as follows<span><sup>2, 3</sup></span>: external defibrillation, deep sedation with intubation, mechanical circulatory support, eliminating causes, intravenous magnesium sulfate irrelevant to the renal dysfunction, correct serum potassium level, isoproterenol infusion, and temporary overdrive pacing.<span><sup>2, 3</sup></span> The dosage of quinolones should be adjusted according to renal function,<span><sup>1</sup></span> and should be prescribed based on age and comorbidities.</p><p>The authors have no conflict of interest to declare.</p><p>Approval of the research protocol: N/A.</p><p>Informed consent: We obtained the informed consent from the patient for the publication of the report.</p><p>Registry and the registration no. of the study/trial: N/A.</p><p>Animal studies: N/A.</p>","PeriodicalId":7196,"journal":{"name":"Acute Medicine & Surgery","volume":"10 1","pages":""},"PeriodicalIF":1.5000,"publicationDate":"2023-12-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ams2.910","citationCount":"0","resultStr":"{\"title\":\"Torsades de pointes due to oral sitafloxacin\",\"authors\":\"Yugo Wakayama, Satoshi Yoshimura, Katsuyuki Hanabusa, Nobuhiro Ikeda, Nobuhiro Miyamae, Yasuyuki Sumida\",\"doi\":\"10.1002/ams2.910\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>A woman aged in her 80s had multiple comorbidities with congestive heart failure, aortic stenosis, and chronic renal failure. The QTc interval 6 months before admission was normal (454 ms) (Figure 1A). Three days pre-admission, the maximum dose of sitafloxacin was prescribed to treat urinary tract infections. She presented with convulsions, a complete atrioventricular block, a prolonged QTc interval (538 ms) (Figure 1B), and recurrent torsade de pointes (TdP) (Figure 1C). Treatment involved 2 g magnesium sulfate infusion, noninvasive positive pressure ventilation, and emergency pacing. After the heart failure management with discontinuation of sitafloxacin, the QTc interval was improved by 501 and 466 ms on day 7 and 20, respectively (Figure 1D,E). She remained healthy at 6-month follow-up. Oral quinolones are commonly prescribed antibiotics in clinical settings<span><sup>1</sup></span>; it could induce QT prolongation as <i>hERG</i> gene class effects on potassium channels and causes TdP, especially in the elderly.<span><sup>1</sup></span> Treatments are as follows<span><sup>2, 3</sup></span>: external defibrillation, deep sedation with intubation, mechanical circulatory support, eliminating causes, intravenous magnesium sulfate irrelevant to the renal dysfunction, correct serum potassium level, isoproterenol infusion, and temporary overdrive pacing.<span><sup>2, 3</sup></span> The dosage of quinolones should be adjusted according to renal function,<span><sup>1</sup></span> and should be prescribed based on age and comorbidities.</p><p>The authors have no conflict of interest to declare.</p><p>Approval of the research protocol: N/A.</p><p>Informed consent: We obtained the informed consent from the patient for the publication of the report.</p><p>Registry and the registration no. of the study/trial: N/A.</p><p>Animal studies: N/A.</p>\",\"PeriodicalId\":7196,\"journal\":{\"name\":\"Acute Medicine & Surgery\",\"volume\":\"10 1\",\"pages\":\"\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2023-12-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ams2.910\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Acute Medicine & Surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ams2.910\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acute Medicine & Surgery","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ams2.910","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
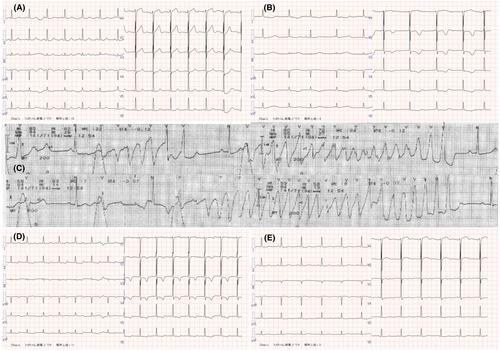
A woman aged in her 80s had multiple comorbidities with congestive heart failure, aortic stenosis, and chronic renal failure. The QTc interval 6 months before admission was normal (454 ms) (Figure 1A). Three days pre-admission, the maximum dose of sitafloxacin was prescribed to treat urinary tract infections. She presented with convulsions, a complete atrioventricular block, a prolonged QTc interval (538 ms) (Figure 1B), and recurrent torsade de pointes (TdP) (Figure 1C). Treatment involved 2 g magnesium sulfate infusion, noninvasive positive pressure ventilation, and emergency pacing. After the heart failure management with discontinuation of sitafloxacin, the QTc interval was improved by 501 and 466 ms on day 7 and 20, respectively (Figure 1D,E). She remained healthy at 6-month follow-up. Oral quinolones are commonly prescribed antibiotics in clinical settings1; it could induce QT prolongation as hERG gene class effects on potassium channels and causes TdP, especially in the elderly.1 Treatments are as follows2, 3: external defibrillation, deep sedation with intubation, mechanical circulatory support, eliminating causes, intravenous magnesium sulfate irrelevant to the renal dysfunction, correct serum potassium level, isoproterenol infusion, and temporary overdrive pacing.2, 3 The dosage of quinolones should be adjusted according to renal function,1 and should be prescribed based on age and comorbidities.
The authors have no conflict of interest to declare.
Approval of the research protocol: N/A.
Informed consent: We obtained the informed consent from the patient for the publication of the report.
Registry and the registration no. of the study/trial: N/A.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


