Padam Kanta Dahal, Lal Rawal, Zanfina Ademi, Rashidul Alam Mahumud, Grish Paudel, Corneel Vandelanotte
{"title":"估算尼泊尔管理和护理 2 型糖尿病的医疗开支:患者视角。","authors":"Padam Kanta Dahal, Lal Rawal, Zanfina Ademi, Rashidul Alam Mahumud, Grish Paudel, Corneel Vandelanotte","doi":"10.1177/23814683231216938","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background.</b> This study aimed to estimate the health care expenditure for managing type 2 diabetes (T2D) in the community setting of Nepal. <b>Methods.</b> This is a baseline cross-sectional study of a heath behavior intervention that was conducted between September 2021 and February 2022 among patients with T2D (<i>N</i> = 481) in the Kavrepalanchok and Nuwakot districts of Nepal. Bottom-up and micro-costing approaches were used to estimate the health care costs and were stratified according to residential status and the presence of comorbid conditions. A generalized linear model with a log-link and gamma distribution was applied for modeling the continuous right-skewed costs, and 95% confidence intervals were obtained from 10,000 bootstrapping resampling techniques. <b>Results.</b> Over 6 months the mean health care resource cost to manage T2D was US $22.87 per patient: 61% included the direct medical cost (US $14.01), 15% included the direct nonmedical cost (US $3.43), and 24% was associated with productivity losses (US $5.44). The mean health care resource cost per patient living in an urban community (US $24.65) was about US $4.95 higher than patients living in the rural community (US $19.69). The health care costs per patient with comorbid conditions was US $22.93 and was US $22.81 for those without comorbidities. Patients living in rural areas had 16% lower health care expenses compared with their urban counterparts. <b>Conclusion.</b> T2D imposes a substantial financial burden on both the health care system and individuals. There is a need to establish high-value care treatment strategies for the management of T2D to reduce the high health care expenses.</p><p><strong>Highlights: </strong>More than 60% of health care expenses comprise the direct medical cost, 15% direct nonmedical cost, and 24% patient productivity losses. The costs of diagnosis, hospitalization, and recommended foods were the main drivers of health care costs for managing type 2 diabetes.Health care expenses among patients living in urban communities and patients with comorbid conditions was higher compared with those in rural communities and those with without comorbidities.The results of this study are expected to help integrate diabetes care within the existing primary health care systems, thereby reducing health care expenses and improving the quality of diabetes care in Nepal.</p>","PeriodicalId":36567,"journal":{"name":"MDM Policy and Practice","volume":"8 2","pages":"23814683231216938"},"PeriodicalIF":1.7000,"publicationDate":"2023-12-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10725113/pdf/","citationCount":"0","resultStr":"{\"title\":\"Estimating the Health Care Expenditure to Manage and Care for Type 2 Diabetes in Nepal: A Patient Perspective.\",\"authors\":\"Padam Kanta Dahal, Lal Rawal, Zanfina Ademi, Rashidul Alam Mahumud, Grish Paudel, Corneel Vandelanotte\",\"doi\":\"10.1177/23814683231216938\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background.</b> This study aimed to estimate the health care expenditure for managing type 2 diabetes (T2D) in the community setting of Nepal. <b>Methods.</b> This is a baseline cross-sectional study of a heath behavior intervention that was conducted between September 2021 and February 2022 among patients with T2D (<i>N</i> = 481) in the Kavrepalanchok and Nuwakot districts of Nepal. Bottom-up and micro-costing approaches were used to estimate the health care costs and were stratified according to residential status and the presence of comorbid conditions. A generalized linear model with a log-link and gamma distribution was applied for modeling the continuous right-skewed costs, and 95% confidence intervals were obtained from 10,000 bootstrapping resampling techniques. <b>Results.</b> Over 6 months the mean health care resource cost to manage T2D was US $22.87 per patient: 61% included the direct medical cost (US $14.01), 15% included the direct nonmedical cost (US $3.43), and 24% was associated with productivity losses (US $5.44). The mean health care resource cost per patient living in an urban community (US $24.65) was about US $4.95 higher than patients living in the rural community (US $19.69). The health care costs per patient with comorbid conditions was US $22.93 and was US $22.81 for those without comorbidities. Patients living in rural areas had 16% lower health care expenses compared with their urban counterparts. <b>Conclusion.</b> T2D imposes a substantial financial burden on both the health care system and individuals. There is a need to establish high-value care treatment strategies for the management of T2D to reduce the high health care expenses.</p><p><strong>Highlights: </strong>More than 60% of health care expenses comprise the direct medical cost, 15% direct nonmedical cost, and 24% patient productivity losses. The costs of diagnosis, hospitalization, and recommended foods were the main drivers of health care costs for managing type 2 diabetes.Health care expenses among patients living in urban communities and patients with comorbid conditions was higher compared with those in rural communities and those with without comorbidities.The results of this study are expected to help integrate diabetes care within the existing primary health care systems, thereby reducing health care expenses and improving the quality of diabetes care in Nepal.</p>\",\"PeriodicalId\":36567,\"journal\":{\"name\":\"MDM Policy and Practice\",\"volume\":\"8 2\",\"pages\":\"23814683231216938\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2023-12-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10725113/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"MDM Policy and Practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/23814683231216938\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"MDM Policy and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/23814683231216938","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/7/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
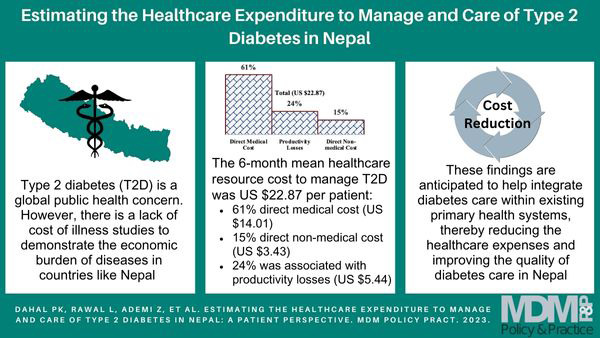
Estimating the Health Care Expenditure to Manage and Care for Type 2 Diabetes in Nepal: A Patient Perspective.
Background. This study aimed to estimate the health care expenditure for managing type 2 diabetes (T2D) in the community setting of Nepal. Methods. This is a baseline cross-sectional study of a heath behavior intervention that was conducted between September 2021 and February 2022 among patients with T2D (N = 481) in the Kavrepalanchok and Nuwakot districts of Nepal. Bottom-up and micro-costing approaches were used to estimate the health care costs and were stratified according to residential status and the presence of comorbid conditions. A generalized linear model with a log-link and gamma distribution was applied for modeling the continuous right-skewed costs, and 95% confidence intervals were obtained from 10,000 bootstrapping resampling techniques. Results. Over 6 months the mean health care resource cost to manage T2D was US $22.87 per patient: 61% included the direct medical cost (US $14.01), 15% included the direct nonmedical cost (US $3.43), and 24% was associated with productivity losses (US $5.44). The mean health care resource cost per patient living in an urban community (US $24.65) was about US $4.95 higher than patients living in the rural community (US $19.69). The health care costs per patient with comorbid conditions was US $22.93 and was US $22.81 for those without comorbidities. Patients living in rural areas had 16% lower health care expenses compared with their urban counterparts. Conclusion. T2D imposes a substantial financial burden on both the health care system and individuals. There is a need to establish high-value care treatment strategies for the management of T2D to reduce the high health care expenses.
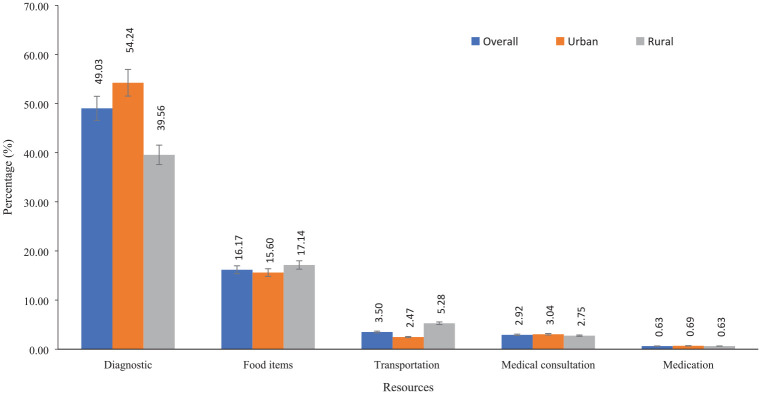
Highlights: More than 60% of health care expenses comprise the direct medical cost, 15% direct nonmedical cost, and 24% patient productivity losses. The costs of diagnosis, hospitalization, and recommended foods were the main drivers of health care costs for managing type 2 diabetes.Health care expenses among patients living in urban communities and patients with comorbid conditions was higher compared with those in rural communities and those with without comorbidities.The results of this study are expected to help integrate diabetes care within the existing primary health care systems, thereby reducing health care expenses and improving the quality of diabetes care in Nepal.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


