Rhodri Saunders, Rafael Torrejon Torres, Henning Reuter, Scott Gibson
{"title":"探索德国髋关节和膝关节置换术中使用手术部位感染预防包的成本后果的卫生经济分析。","authors":"Rhodri Saunders, Rafael Torrejon Torres, Henning Reuter, Scott Gibson","doi":"10.36469/001c.90651","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>According to the European Centre for Disease Prevention and Control, surgical site infections (SSIs) constitute over 50% of all hospital-acquired infections. Reducing SSIs can enhance healthcare efficiency.</p><p><strong>Objective: </strong>This study explores the cost consequences of implementing an SSI prevention bundle (SPB) in total hip and knee arthroplasty (THKA).</p><p><strong>Methods: </strong>A health-economic model followed a cohort of THKA patients from admission to 90 days postdischarge. The perioperative process was modeled using a decision tree, and postoperative recovery and potential SSI evaluated using a Markov model. The model reflects the hospital payers' perspective in Germany. The SPB includes antimicrobial incision drapes, patient warming, and negative pressure wound therapy in high-risk patients. SSI reduction associated with these interventions was sourced from published meta-analyses. An effectiveness factor of 70% was introduced to account for potential overlap of effectiveness when interventions are used in combination. Sensitivity analyses were performed to assess the robustness of model outcomes.</p><p><strong>Results: </strong>The cost with the SPB was €4274.32 per patient, €98.27, or 2.25%, lower than that of the standard of care (€4372.59). Sensitivity analyses confirmed these findings, indicating a median saving of 2.22% (95% credible interval: 1.00%-3.79%]). The SPB also reduced inpatient SSI incidence from 2.96% to 0.91%. The break-even point for the SPB was found when the standard of care had an SSI incidence of 0.938%. Major cost drivers were the cost of inpatient SSI care, general ward, and operating room, and the increased risk of an SSI associated with unintended, intraoperative hypothermia. Varying the effectiveness factor from 10% to 130% did not substantially impact model outcomes.</p><p><strong>Conclusions: </strong>Introducing the SPB is expected to reduce care costs if the inpatient SSI rate (superficial and deep combined) in THKA procedures exceeds 1%. Research into how bundles of measures perform together is required to further inform the results of this computational analysis.</p>","PeriodicalId":16012,"journal":{"name":"Journal of Health Economics and Outcomes Research","volume":"10 2","pages":"132-140"},"PeriodicalIF":2.3000,"publicationDate":"2023-12-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10720700/pdf/","citationCount":"0","resultStr":"{\"title\":\"A Health Economic Analysis Exploring the Cost Consequence of Using a Surgical Site Infection Prevention Bundle for Hip and Knee Arthroplasty in Germany.\",\"authors\":\"Rhodri Saunders, Rafael Torrejon Torres, Henning Reuter, Scott Gibson\",\"doi\":\"10.36469/001c.90651\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>According to the European Centre for Disease Prevention and Control, surgical site infections (SSIs) constitute over 50% of all hospital-acquired infections. Reducing SSIs can enhance healthcare efficiency.</p><p><strong>Objective: </strong>This study explores the cost consequences of implementing an SSI prevention bundle (SPB) in total hip and knee arthroplasty (THKA).</p><p><strong>Methods: </strong>A health-economic model followed a cohort of THKA patients from admission to 90 days postdischarge. The perioperative process was modeled using a decision tree, and postoperative recovery and potential SSI evaluated using a Markov model. The model reflects the hospital payers' perspective in Germany. The SPB includes antimicrobial incision drapes, patient warming, and negative pressure wound therapy in high-risk patients. SSI reduction associated with these interventions was sourced from published meta-analyses. An effectiveness factor of 70% was introduced to account for potential overlap of effectiveness when interventions are used in combination. Sensitivity analyses were performed to assess the robustness of model outcomes.</p><p><strong>Results: </strong>The cost with the SPB was €4274.32 per patient, €98.27, or 2.25%, lower than that of the standard of care (€4372.59). Sensitivity analyses confirmed these findings, indicating a median saving of 2.22% (95% credible interval: 1.00%-3.79%]). The SPB also reduced inpatient SSI incidence from 2.96% to 0.91%. The break-even point for the SPB was found when the standard of care had an SSI incidence of 0.938%. Major cost drivers were the cost of inpatient SSI care, general ward, and operating room, and the increased risk of an SSI associated with unintended, intraoperative hypothermia. Varying the effectiveness factor from 10% to 130% did not substantially impact model outcomes.</p><p><strong>Conclusions: </strong>Introducing the SPB is expected to reduce care costs if the inpatient SSI rate (superficial and deep combined) in THKA procedures exceeds 1%. Research into how bundles of measures perform together is required to further inform the results of this computational analysis.</p>\",\"PeriodicalId\":16012,\"journal\":{\"name\":\"Journal of Health Economics and Outcomes Research\",\"volume\":\"10 2\",\"pages\":\"132-140\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2023-12-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10720700/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Health Economics and Outcomes Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.36469/001c.90651\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"ECONOMICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Health Economics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.36469/001c.90651","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ECONOMICS","Score":null,"Total":0}
A Health Economic Analysis Exploring the Cost Consequence of Using a Surgical Site Infection Prevention Bundle for Hip and Knee Arthroplasty in Germany.
Background: According to the European Centre for Disease Prevention and Control, surgical site infections (SSIs) constitute over 50% of all hospital-acquired infections. Reducing SSIs can enhance healthcare efficiency.
Objective: This study explores the cost consequences of implementing an SSI prevention bundle (SPB) in total hip and knee arthroplasty (THKA).
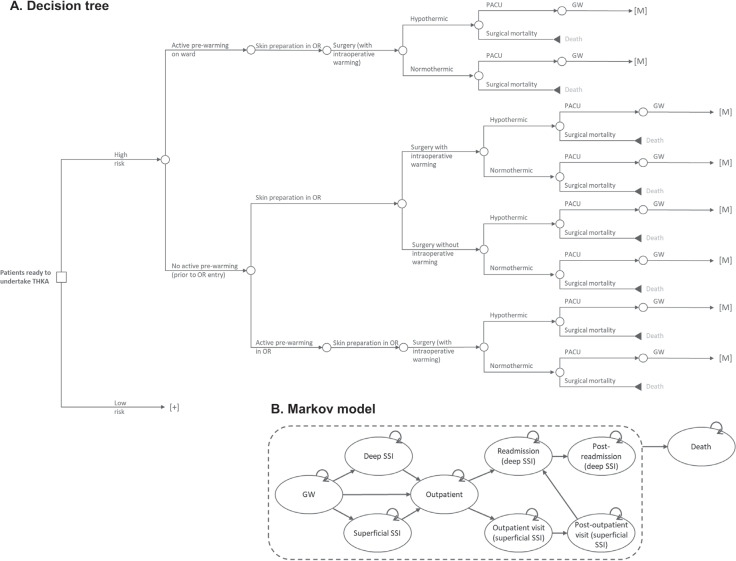
Methods: A health-economic model followed a cohort of THKA patients from admission to 90 days postdischarge. The perioperative process was modeled using a decision tree, and postoperative recovery and potential SSI evaluated using a Markov model. The model reflects the hospital payers' perspective in Germany. The SPB includes antimicrobial incision drapes, patient warming, and negative pressure wound therapy in high-risk patients. SSI reduction associated with these interventions was sourced from published meta-analyses. An effectiveness factor of 70% was introduced to account for potential overlap of effectiveness when interventions are used in combination. Sensitivity analyses were performed to assess the robustness of model outcomes.
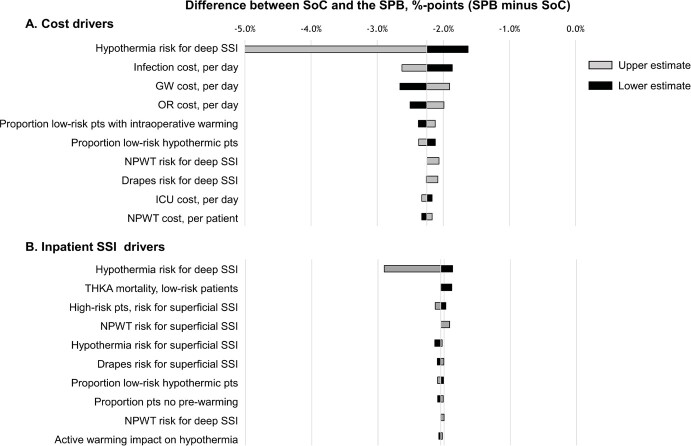
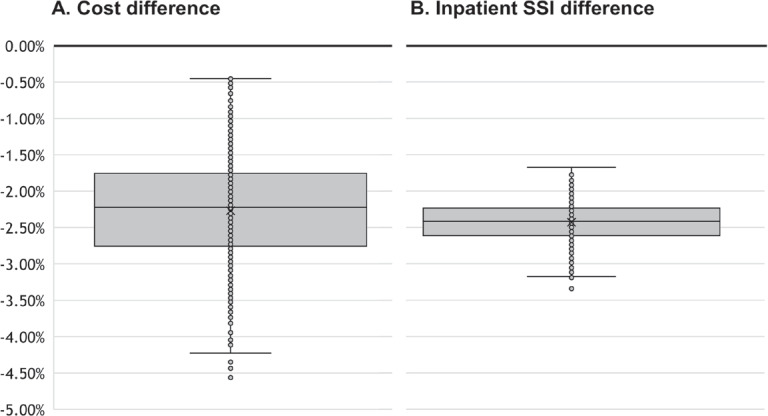
Results: The cost with the SPB was €4274.32 per patient, €98.27, or 2.25%, lower than that of the standard of care (€4372.59). Sensitivity analyses confirmed these findings, indicating a median saving of 2.22% (95% credible interval: 1.00%-3.79%]). The SPB also reduced inpatient SSI incidence from 2.96% to 0.91%. The break-even point for the SPB was found when the standard of care had an SSI incidence of 0.938%. Major cost drivers were the cost of inpatient SSI care, general ward, and operating room, and the increased risk of an SSI associated with unintended, intraoperative hypothermia. Varying the effectiveness factor from 10% to 130% did not substantially impact model outcomes.
Conclusions: Introducing the SPB is expected to reduce care costs if the inpatient SSI rate (superficial and deep combined) in THKA procedures exceeds 1%. Research into how bundles of measures perform together is required to further inform the results of this computational analysis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


