Michael Arndt, Hans Lippert, Roland S Croner, Frank Meyer, Ronny Otto, Karsten Ridwelski
{"title":"晚期结肠癌和直肠癌多脏器切除:一项前瞻性多中心观察性研究,对发病率、死亡率和生存率进行倾向评分分析。","authors":"Michael Arndt, Hans Lippert, Roland S Croner, Frank Meyer, Ronny Otto, Karsten Ridwelski","doi":"10.1515/iss-2023-0027","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>In the surgical treatment of colorectal carcinoma (CRC), 1 in 10 patients has a peritumorous adhesion or tumor infiltration in the adjacent tissue or organs. Accordingly, multivisceral resection (MVR) must be performed in these patients. This prospective multicenter observational study aimed to analyze the possible differences between non-multivisceral resection (nMVR) and MVR in terms of early postoperative and long-term oncological treatment outcomes. We also aimed to determine the factors influencing overall survival.</p><p><strong>Methods: </strong>The data of 25,321 patients from 364 hospitals who had undergone surgery for CRC (the Union for International Cancer Control stages I-III) during a defined period were evaluated. MVR was defined as (partial) resection of the tumor-bearing organ along with resection of the adherent and adjacent organs or tissues. In addition to the patients' personal, diagnosis (tumor findings), and therapy data, demographic data were also recorded and the early postoperative outcome was determined. Furthermore, the long-term survival of each patient was investigated, and a \"matched-pair\" analysis was performed.</p><p><strong>Results: </strong>From 2008 to 2015, the MVR rates were 9.9 % (n=1,551) for colon cancer (colon CA) and 10.6 % (n=1,027) for rectal cancer (rectal CA). CRC was more common in men (colon CA: 53.4 %; rectal CA: 62.0 %) than in women; all MVR groups had high proportions of women (53.6 % vs. 55.2 %; pairs of values in previously mentioned order). Resection of another organ frequently occurred (75.6 % vs. 63.7 %). The MVR group had a high prevalence of intraoperative (5.8 %; 12.1 %) and postoperative surgical complications (30.8 % vs. 36.4 %; each p<0.001). Wound infections (colon CA: 7.1 %) and anastomotic insufficiencies (rectal CA: 8.3 %) frequently occurred after MVR. The morbidity rates of the MVR groups were also determined (43.7 % vs. 47.2 %). The hospital mortality rates were 4.9 % in the colon CA-related MVR group and 3.8 % in the rectal CA-related MVR group and were significantly increased compared with those of the nMVR group (both p<0.001). Results of the matched-pair analysis showed that the morbidity rates in both MVR groups (colon CA: 42.9 % vs. 34.3 %; rectal CA: 46.3 % vs. 37.2 %; each p<0.001) were significantly increased. The hospital lethality rate tended to increase in the colon CA-related MVR group (4.8 % vs. 3.7 %; p=0.084), while it significantly increased in the rectal CA-related MVR group (3.4 % vs. 3.0 %; p=0.005). Moreover, the 5-year (yr) overall survival rates were 53.9 % (nMVR: 69.5 %; p<0.001) in the colon CA group and 56.8 % (nMVR: 69.4 %; p<0.001) in the rectal CA group. Comparison of individual T stages (MVR vs. nMVR) showed no significant differences in the survival outcomes (p<0.05); however, according to the matched-pair analysis, a significant difference was observed in the survival outcomes of those with pT4 colon CA (40.6 % vs. 50.2 %; p=0.017). By contrast, the local recurrence rates after MVR were not significantly different (7.0 % vs. 5.8 %; both p>0.05). The risk factors common to both tumor types were advanced age (>79 yr), pT stage, sex, and morbidity (each hazard ratio: >1; p<0.05).</p><p><strong>Conclusions: </strong>MVR allows curation by R0 resection with adequate long-term survival. For colon or rectal CA, MVR tended to be associated with reduced 5-year overall survival rates (significant only for pT4 colon CA based on the MPA results), as well as, with a significant increase in morbidity rates in both tumor entities. In the overall data, MVR was associated with significant increases in hospital lethality rates, as indicated by the matched-pair analysis (significant only for rectal CA).</p>","PeriodicalId":44186,"journal":{"name":"Innovative Surgical Sciences","volume":"8 2","pages":"61-72"},"PeriodicalIF":1.2000,"publicationDate":"2023-11-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10696939/pdf/","citationCount":"0","resultStr":"{\"title\":\"Multivisceral resection of advanced colon and rectal cancer: a prospective multicenter observational study with propensity score analysis of the morbidity, mortality, and survival.\",\"authors\":\"Michael Arndt, Hans Lippert, Roland S Croner, Frank Meyer, Ronny Otto, Karsten Ridwelski\",\"doi\":\"10.1515/iss-2023-0027\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>In the surgical treatment of colorectal carcinoma (CRC), 1 in 10 patients has a peritumorous adhesion or tumor infiltration in the adjacent tissue or organs. Accordingly, multivisceral resection (MVR) must be performed in these patients. This prospective multicenter observational study aimed to analyze the possible differences between non-multivisceral resection (nMVR) and MVR in terms of early postoperative and long-term oncological treatment outcomes. We also aimed to determine the factors influencing overall survival.</p><p><strong>Methods: </strong>The data of 25,321 patients from 364 hospitals who had undergone surgery for CRC (the Union for International Cancer Control stages I-III) during a defined period were evaluated. MVR was defined as (partial) resection of the tumor-bearing organ along with resection of the adherent and adjacent organs or tissues. In addition to the patients' personal, diagnosis (tumor findings), and therapy data, demographic data were also recorded and the early postoperative outcome was determined. Furthermore, the long-term survival of each patient was investigated, and a \\\"matched-pair\\\" analysis was performed.</p><p><strong>Results: </strong>From 2008 to 2015, the MVR rates were 9.9 % (n=1,551) for colon cancer (colon CA) and 10.6 % (n=1,027) for rectal cancer (rectal CA). CRC was more common in men (colon CA: 53.4 %; rectal CA: 62.0 %) than in women; all MVR groups had high proportions of women (53.6 % vs. 55.2 %; pairs of values in previously mentioned order). Resection of another organ frequently occurred (75.6 % vs. 63.7 %). The MVR group had a high prevalence of intraoperative (5.8 %; 12.1 %) and postoperative surgical complications (30.8 % vs. 36.4 %; each p<0.001). Wound infections (colon CA: 7.1 %) and anastomotic insufficiencies (rectal CA: 8.3 %) frequently occurred after MVR. The morbidity rates of the MVR groups were also determined (43.7 % vs. 47.2 %). The hospital mortality rates were 4.9 % in the colon CA-related MVR group and 3.8 % in the rectal CA-related MVR group and were significantly increased compared with those of the nMVR group (both p<0.001). Results of the matched-pair analysis showed that the morbidity rates in both MVR groups (colon CA: 42.9 % vs. 34.3 %; rectal CA: 46.3 % vs. 37.2 %; each p<0.001) were significantly increased. The hospital lethality rate tended to increase in the colon CA-related MVR group (4.8 % vs. 3.7 %; p=0.084), while it significantly increased in the rectal CA-related MVR group (3.4 % vs. 3.0 %; p=0.005). Moreover, the 5-year (yr) overall survival rates were 53.9 % (nMVR: 69.5 %; p<0.001) in the colon CA group and 56.8 % (nMVR: 69.4 %; p<0.001) in the rectal CA group. Comparison of individual T stages (MVR vs. nMVR) showed no significant differences in the survival outcomes (p<0.05); however, according to the matched-pair analysis, a significant difference was observed in the survival outcomes of those with pT4 colon CA (40.6 % vs. 50.2 %; p=0.017). By contrast, the local recurrence rates after MVR were not significantly different (7.0 % vs. 5.8 %; both p>0.05). The risk factors common to both tumor types were advanced age (>79 yr), pT stage, sex, and morbidity (each hazard ratio: >1; p<0.05).</p><p><strong>Conclusions: </strong>MVR allows curation by R0 resection with adequate long-term survival. For colon or rectal CA, MVR tended to be associated with reduced 5-year overall survival rates (significant only for pT4 colon CA based on the MPA results), as well as, with a significant increase in morbidity rates in both tumor entities. In the overall data, MVR was associated with significant increases in hospital lethality rates, as indicated by the matched-pair analysis (significant only for rectal CA).</p>\",\"PeriodicalId\":44186,\"journal\":{\"name\":\"Innovative Surgical Sciences\",\"volume\":\"8 2\",\"pages\":\"61-72\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2023-11-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10696939/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Innovative Surgical Sciences\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1515/iss-2023-0027\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/6/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Innovative Surgical Sciences","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1515/iss-2023-0027","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/6/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
摘要
目的:在结直肠癌(CRC)的手术治疗中,每10例患者中就有1例存在瘤周粘连或肿瘤浸润邻近组织或器官。因此,这些患者必须进行多脏器切除(MVR)。本前瞻性多中心观察性研究旨在分析非多脏器切除(nMVR)和MVR在术后早期和长期肿瘤治疗结果方面可能存在的差异。我们还旨在确定影响总生存率的因素。方法:对来自364家医院的25321例CRC手术患者(国际癌症控制联盟I-III期)的数据进行评估。MVR的定义是(部分)切除荷瘤器官,同时切除附着和邻近的器官或组织。除了患者的个人、诊断(肿瘤发现)和治疗数据外,还记录了人口统计学数据,并确定了术后早期结局。此外,对每位患者的长期生存进行了调查,并进行了“配对”分析。结果:2008 - 2015年,结肠癌(结肠CA)的MVR率为9.9 % (n= 1551),直肠癌(直肠CA)的MVR率为10.6 % (n= 1027)。结直肠癌在男性中更为常见(结肠CA: 53.4% %;直肠CA: 62.0 %)高于女性;所有MVR组的女性比例都很高(53.6 % vs. 55.2% %;按前面提到的顺序排列的值对)。另一器官的切除经常发生(75.6% % vs. 63.7 %)。MVR组术中发生率高(5.8% %;12.1 %)和术后手术并发症(30.8 % vs 36.4 %;每个p0.05)。两种肿瘤类型的共同危险因素为高龄(>79 yr)、pT分期、性别和发病率(各危险比>1;结论:MVR可以通过R0切除进行治疗,并有足够的长期生存。对于结肠或直肠CA, MVR往往与5年总生存率降低相关(基于MPA结果,仅pT4结肠CA显著),并且两种肿瘤实体的发病率均显著增加。在总体数据中,配对分析表明,MVR与医院死亡率的显著增加相关(仅对直肠CA有显著性)。
Multivisceral resection of advanced colon and rectal cancer: a prospective multicenter observational study with propensity score analysis of the morbidity, mortality, and survival.
Objectives: In the surgical treatment of colorectal carcinoma (CRC), 1 in 10 patients has a peritumorous adhesion or tumor infiltration in the adjacent tissue or organs. Accordingly, multivisceral resection (MVR) must be performed in these patients. This prospective multicenter observational study aimed to analyze the possible differences between non-multivisceral resection (nMVR) and MVR in terms of early postoperative and long-term oncological treatment outcomes. We also aimed to determine the factors influencing overall survival.
Methods: The data of 25,321 patients from 364 hospitals who had undergone surgery for CRC (the Union for International Cancer Control stages I-III) during a defined period were evaluated. MVR was defined as (partial) resection of the tumor-bearing organ along with resection of the adherent and adjacent organs or tissues. In addition to the patients' personal, diagnosis (tumor findings), and therapy data, demographic data were also recorded and the early postoperative outcome was determined. Furthermore, the long-term survival of each patient was investigated, and a "matched-pair" analysis was performed.
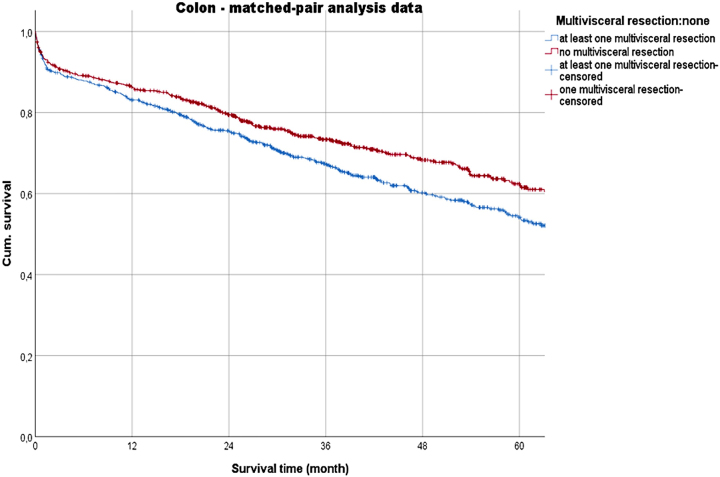
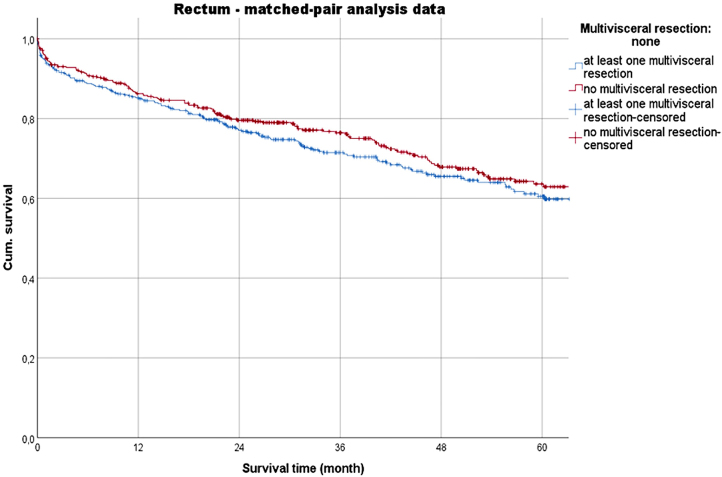
Results: From 2008 to 2015, the MVR rates were 9.9 % (n=1,551) for colon cancer (colon CA) and 10.6 % (n=1,027) for rectal cancer (rectal CA). CRC was more common in men (colon CA: 53.4 %; rectal CA: 62.0 %) than in women; all MVR groups had high proportions of women (53.6 % vs. 55.2 %; pairs of values in previously mentioned order). Resection of another organ frequently occurred (75.6 % vs. 63.7 %). The MVR group had a high prevalence of intraoperative (5.8 %; 12.1 %) and postoperative surgical complications (30.8 % vs. 36.4 %; each p<0.001). Wound infections (colon CA: 7.1 %) and anastomotic insufficiencies (rectal CA: 8.3 %) frequently occurred after MVR. The morbidity rates of the MVR groups were also determined (43.7 % vs. 47.2 %). The hospital mortality rates were 4.9 % in the colon CA-related MVR group and 3.8 % in the rectal CA-related MVR group and were significantly increased compared with those of the nMVR group (both p<0.001). Results of the matched-pair analysis showed that the morbidity rates in both MVR groups (colon CA: 42.9 % vs. 34.3 %; rectal CA: 46.3 % vs. 37.2 %; each p<0.001) were significantly increased. The hospital lethality rate tended to increase in the colon CA-related MVR group (4.8 % vs. 3.7 %; p=0.084), while it significantly increased in the rectal CA-related MVR group (3.4 % vs. 3.0 %; p=0.005). Moreover, the 5-year (yr) overall survival rates were 53.9 % (nMVR: 69.5 %; p<0.001) in the colon CA group and 56.8 % (nMVR: 69.4 %; p<0.001) in the rectal CA group. Comparison of individual T stages (MVR vs. nMVR) showed no significant differences in the survival outcomes (p<0.05); however, according to the matched-pair analysis, a significant difference was observed in the survival outcomes of those with pT4 colon CA (40.6 % vs. 50.2 %; p=0.017). By contrast, the local recurrence rates after MVR were not significantly different (7.0 % vs. 5.8 %; both p>0.05). The risk factors common to both tumor types were advanced age (>79 yr), pT stage, sex, and morbidity (each hazard ratio: >1; p<0.05).
Conclusions: MVR allows curation by R0 resection with adequate long-term survival. For colon or rectal CA, MVR tended to be associated with reduced 5-year overall survival rates (significant only for pT4 colon CA based on the MPA results), as well as, with a significant increase in morbidity rates in both tumor entities. In the overall data, MVR was associated with significant increases in hospital lethality rates, as indicated by the matched-pair analysis (significant only for rectal CA).

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


