Eleni Stamellou, Claudia Seikrit, Sydney C W Tang, Peter Boor, Vladimir Tesař, Jürgen Floege, Jonathan Barratt, Rafael Kramann
{"title":"IgA nephropathy。","authors":"Eleni Stamellou, Claudia Seikrit, Sydney C W Tang, Peter Boor, Vladimir Tesař, Jürgen Floege, Jonathan Barratt, Rafael Kramann","doi":"10.1038/s41572-023-00476-9","DOIUrl":null,"url":null,"abstract":"<p><p>IgA nephropathy (IgAN), the most prevalent primary glomerulonephritis worldwide, carries a considerable lifetime risk of kidney failure. Clinical manifestations of IgAN vary from asymptomatic with microscopic or intermittent macroscopic haematuria and stable kidney function to rapidly progressive glomerulonephritis. IgAN has been proposed to develop through a 'four-hit' process, commencing with overproduction and increased systemic presence of poorly O-glycosylated galactose-deficient IgA1 (Gd-IgA1), followed by recognition of Gd-IgA1 by antiglycan autoantibodies, aggregation of Gd-IgA1 and formation of polymeric IgA1 immune complexes and, lastly, deposition of these immune complexes in the glomerular mesangium, leading to kidney inflammation and scarring. IgAN can only be diagnosed by kidney biopsy. Extensive, optimized supportive care is the mainstay of therapy for patients with IgAN. For those at high risk of disease progression, the 2021 KDIGO Clinical Practice Guideline suggests considering a 6-month course of systemic corticosteroid therapy; however, the efficacy of systemic steroid treatment is under debate and serious adverse effects are common. Advances in understanding the pathophysiology of IgAN have led to clinical trials of novel targeted therapies with acceptable safety profiles, including SGLT2 inhibitors, endothelin receptor blockers, targeted-release budesonide, B cell proliferation and differentiation inhibitors, as well as blockade of complement components.</p>","PeriodicalId":18910,"journal":{"name":"Nature Reviews Disease Primers","volume":null,"pages":null},"PeriodicalIF":76.9000,"publicationDate":"2023-11-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"IgA nephropathy.\",\"authors\":\"Eleni Stamellou, Claudia Seikrit, Sydney C W Tang, Peter Boor, Vladimir Tesař, Jürgen Floege, Jonathan Barratt, Rafael Kramann\",\"doi\":\"10.1038/s41572-023-00476-9\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>IgA nephropathy (IgAN), the most prevalent primary glomerulonephritis worldwide, carries a considerable lifetime risk of kidney failure. Clinical manifestations of IgAN vary from asymptomatic with microscopic or intermittent macroscopic haematuria and stable kidney function to rapidly progressive glomerulonephritis. IgAN has been proposed to develop through a 'four-hit' process, commencing with overproduction and increased systemic presence of poorly O-glycosylated galactose-deficient IgA1 (Gd-IgA1), followed by recognition of Gd-IgA1 by antiglycan autoantibodies, aggregation of Gd-IgA1 and formation of polymeric IgA1 immune complexes and, lastly, deposition of these immune complexes in the glomerular mesangium, leading to kidney inflammation and scarring. IgAN can only be diagnosed by kidney biopsy. Extensive, optimized supportive care is the mainstay of therapy for patients with IgAN. For those at high risk of disease progression, the 2021 KDIGO Clinical Practice Guideline suggests considering a 6-month course of systemic corticosteroid therapy; however, the efficacy of systemic steroid treatment is under debate and serious adverse effects are common. Advances in understanding the pathophysiology of IgAN have led to clinical trials of novel targeted therapies with acceptable safety profiles, including SGLT2 inhibitors, endothelin receptor blockers, targeted-release budesonide, B cell proliferation and differentiation inhibitors, as well as blockade of complement components.</p>\",\"PeriodicalId\":18910,\"journal\":{\"name\":\"Nature Reviews Disease Primers\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":76.9000,\"publicationDate\":\"2023-11-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Nature Reviews Disease Primers\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1038/s41572-023-00476-9\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Nature Reviews Disease Primers","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1038/s41572-023-00476-9","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
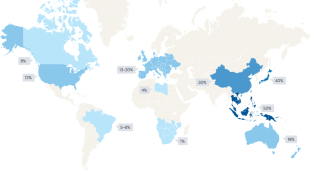
IgA nephropathy (IgAN), the most prevalent primary glomerulonephritis worldwide, carries a considerable lifetime risk of kidney failure. Clinical manifestations of IgAN vary from asymptomatic with microscopic or intermittent macroscopic haematuria and stable kidney function to rapidly progressive glomerulonephritis. IgAN has been proposed to develop through a 'four-hit' process, commencing with overproduction and increased systemic presence of poorly O-glycosylated galactose-deficient IgA1 (Gd-IgA1), followed by recognition of Gd-IgA1 by antiglycan autoantibodies, aggregation of Gd-IgA1 and formation of polymeric IgA1 immune complexes and, lastly, deposition of these immune complexes in the glomerular mesangium, leading to kidney inflammation and scarring. IgAN can only be diagnosed by kidney biopsy. Extensive, optimized supportive care is the mainstay of therapy for patients with IgAN. For those at high risk of disease progression, the 2021 KDIGO Clinical Practice Guideline suggests considering a 6-month course of systemic corticosteroid therapy; however, the efficacy of systemic steroid treatment is under debate and serious adverse effects are common. Advances in understanding the pathophysiology of IgAN have led to clinical trials of novel targeted therapies with acceptable safety profiles, including SGLT2 inhibitors, endothelin receptor blockers, targeted-release budesonide, B cell proliferation and differentiation inhibitors, as well as blockade of complement components.
期刊介绍:
Nature Reviews Disease Primers, a part of the Nature Reviews journal portfolio, features sections on epidemiology, mechanisms, diagnosis, management, and patient quality of life. The editorial team commissions top researchers — comprising basic scientists and clinical researchers — to write the Primers, which are designed for use by early career researchers, medical students and principal investigators. Each Primer concludes with an Outlook section, highlighting future research directions. Covered medical specialties include Cardiology, Dermatology, Ear, Nose and Throat, Emergency Medicine, Endocrinology, Gastroenterology, Genetic Conditions, Gynaecology and Obstetrics, Hepatology, Haematology, Infectious Diseases, Maxillofacial and Oral Medicine, Nephrology, Neurology, Nutrition, Oncology, Ophthalmology, Orthopaedics, Psychiatry, Respiratory Medicine, Rheumatology, Sleep Medicine, and Urology.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


