Vidya L. Ambati, Tammy H. Cummings, Praveen Yerramothu, Joseph Nguyen, S. Scott Sutton, Brian C. Werner, Joseph Magagnoli
{"title":"氟哌啶醇使用与类风湿关节炎风险之间的关系","authors":"Vidya L. Ambati, Tammy H. Cummings, Praveen Yerramothu, Joseph Nguyen, S. Scott Sutton, Brian C. Werner, Joseph Magagnoli","doi":"10.1002/mef2.66","DOIUrl":null,"url":null,"abstract":"<p>An uncontrolled case-series reported a benefit of haloperidol in rheumatoid arthritis (RA).<span><sup>1</sup></span> A study of the FDA Adverse Events Reporting System reported that among RA patients there were fewer users of antipsychotic drugs, including haloperidol, and concluded that antipsychotic drugs could reduce the risk of developing RA.<span><sup>2</sup></span> However, these results only suggest the converse: that RA is associated with a reduced risk of antipsychotic use; they do not indicate that antipsychotics reduce the risk of RA. The same study also examined a small employee insurance database in Japan and reported an inverse temporal relationship between RA and antipsychotic drugs, including haloperidol. Limitations of these two studies include small size, unverified and incomplete records, lack of correction for sociodemographic or clinical confounders, changing time-trends in prescriptions, and selective loss to follow-up. Therefore, we sought to undertake a robust pharmacoepidemiologic study of whether haloperidol, an FDA-approved drug for the treatment of schizophrenia or Tourette disorder, affects the risk of incident RA in three large nationwide health insurance databases that comprise most of the United States population. We did so with the goal of determining whether an inexpensive drug already in clinical use could be repurposed for RA, a disease that affects tens of millions of people worldwide.</p><p>We studied three health insurance databases: PearlDiver Mariner (2010–2021), IBM Marketscan Research Databases (2006–2020), and Veterans Administration (VA) Health database (2001–2021) (Supporting Information: Tables S1–S4). Inclusion criteria were at least 6 months follow-up, at least 18 years of age, schizophrenia or Tourette disorder diagnosed on two separate occasions, and treatment with antipsychotics. RA before diagnosis of schizophrenia or Tourette disorder was exclusionary (Supporting Information: Figure S1). Disease claims were identified by ICD-9-CM and ICD-10-CM codes. Drug exposure was determined by prescriptions for generic or brand versions. Time from first prescription of antipsychotics to diagnosis of RA was the dependent variable. Sensitivity analyses were performed using diagnosis of schizophrenia or Tourette disorder as the index date and flagging treatment with antipsychotics within 60 days of schizophrenia or Tourette disorder diagnosis. Patients were censored when they developed RA, unenrolled, died, or switched between study medication groups. Cox proportional hazards regression analyses were performed to estimate the hazard of RA in relation to haloperidol use. We performed propensity score matching to create cohorts with similar baseline characteristics, reducing possible bias in estimating treatment effects. Additionally, to control for any residual covariate imbalance, we adjusted for RA-associated confounders: age, sex, smoking, body mass index, Charlson comorbidity index, and database entry year. Fine-Gray subdistribution hazard ratios for competing risk of mortality, corrected for covariates, were calculated for the VA, which contains mortality data. We performed inverse-variance weighted meta-analyses to estimate the combined hazard ratio (HR) and 95% confidence intervals (CI) using a random-effects model, computed prediction intervals, and Kaplan–Meier survival analyses.</p><p>The adjusted Cox proportional hazards regression models in the propensity-score-matched populations showed a protective association of haloperidol use against incident RA in each of the three databases (Figure 1A,B). The meta-analyses identified a protective effect of haloperidol in the main (pooled adjusted hazard ratio [aHR] = 0.69; 95% CI: 0.61–0.79; <i>p</i> = 0.0001) and sensitivity analyses (pooled aHR = 0.69; 95% CI: 0.58–0.81; <i>p</i> < 0.0001) (Figure 1A,B). The 95% prediction intervals for the hazard ratio, which provide insights into the range of outcomes in a hypothetical future study, were <1.0 in both analyses (Figure 1A,B), implying a future clinical trial would be estimated to have a >95% probability of identifying a protective effect. Subdistribution hazard ratios, accounting for the competing risk of mortality, in the VA revealed a protective effect (main analysis: aHR = 0.52; 95% CI: 0.27–0.98; <i>p</i> = 0.0002; sensitivity analysis: aHR = 0.48; 95% CI: 0.30–0.76; <i>p</i> = 0.0002). Kaplan–Meier survival analyses revealed that haloperidol use was associated with a lower risk of incident RA in all three databases in both analyses (Figure 1C,D).</p><p>We identified a significant association between haloperidol use and incident RA. Strengths of our study include replication in three cohorts that comprise most United States adults, adjustment for confounders, and propensity score matching, which simulates randomization and increases its validity. As this retrospective study was not randomized, there could be residual confounding or selection bias.</p><p>Haloperidol is reported to inhibit the cytokines interleukin-1β (IL-1β), IL-6, and tumor necrosis factor-α,<span><sup>3, 4</sup></span> which are known drivers of RA.<span><sup>5</sup></span> Dendritic cells and T helper 1 lymphocytes play crucial roles in the pathogenesis of RA.<span><sup>6</sup></span> Haloperidol suppresses the maturation and priming of these cells, respectively.<span><sup>7</sup></span> Together, such effects could, in part, underlie the mechanistic basis of how haloperidol exposure reduces the development of RA. Clinical studies in individuals with mental illness may face ethical challenges as well as recruitment challenges owing to the incidence in this population. However, taken together with the anti-inflammatory effects of haloperidol, our findings, which suggest a potential benefit of haloperidol in RA, provide a rationale for randomized controlled trials in a general population at risk for RA. Such prospective trials could provide causal insights.</p><p><b>Vidya L. Ambati</b>: Conceptualization (equal); data curation (equal); formal analysis (equal); funding acquisition (equal); methodology (equal); writing—original draft (equal); writing—review & editing (equal). <b>Tammy H. Cummings</b>: Methodology (equal); writing—review and editing (equal). <b>Praveen Yerramothu</b>: Data curation (equal); writing—review and editing (equal). <b>Joseph Nguyen</b>: Data curation (equal); writing—review and editing. <b>S. Scott Sutton</b>: Data curation (equal); funding acquisition; methodology (equal); writing—original draft (equal); writing—review and editing. <b>Brian C. Werner</b>: Conceptualization (equal); data curation (equal); funding acquisition; methodology (equal); supervision (equal); writing—original draft (equal); writing—review and editing. <b>Joseph Magagnoli</b>: Conceptualization (equal); data curation (equal); formal analysis (equal); funding acquisition; methodology (equal); supervision (equal); writing—original draft (equal); writing—review and editing (equal). All authors have read and approved the final manuscript.</p><p>S. Scott Sutton has received research grants from Boehringer Ingelheim, Coherus BioSciences, EMD Serono, and Alexion Pharmaceuticals, all for projects unrelated to study. Brian C. Werner and Vidya L. Ambati are named as inventors on matter-related patent applications filed by their university.</p><p>PearlDiver Mariner and IBM Marketscan Research Databases contained deidentified data deemed exempt by the University of Virginia Institutional Review Board (IRB). Veterans Administration (VA) Health database data analysis was compliant with Department of Veterans Affairs requirements and received IRB (1139248-1) and Research and Development Approval.</p>","PeriodicalId":74135,"journal":{"name":"MedComm - Future medicine","volume":"2 4","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2023-11-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/mef2.66","citationCount":"0","resultStr":"{\"title\":\"Association between haloperidol use and risk of rheumatoid arthritis\",\"authors\":\"Vidya L. Ambati, Tammy H. Cummings, Praveen Yerramothu, Joseph Nguyen, S. Scott Sutton, Brian C. Werner, Joseph Magagnoli\",\"doi\":\"10.1002/mef2.66\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>An uncontrolled case-series reported a benefit of haloperidol in rheumatoid arthritis (RA).<span><sup>1</sup></span> A study of the FDA Adverse Events Reporting System reported that among RA patients there were fewer users of antipsychotic drugs, including haloperidol, and concluded that antipsychotic drugs could reduce the risk of developing RA.<span><sup>2</sup></span> However, these results only suggest the converse: that RA is associated with a reduced risk of antipsychotic use; they do not indicate that antipsychotics reduce the risk of RA. The same study also examined a small employee insurance database in Japan and reported an inverse temporal relationship between RA and antipsychotic drugs, including haloperidol. Limitations of these two studies include small size, unverified and incomplete records, lack of correction for sociodemographic or clinical confounders, changing time-trends in prescriptions, and selective loss to follow-up. Therefore, we sought to undertake a robust pharmacoepidemiologic study of whether haloperidol, an FDA-approved drug for the treatment of schizophrenia or Tourette disorder, affects the risk of incident RA in three large nationwide health insurance databases that comprise most of the United States population. We did so with the goal of determining whether an inexpensive drug already in clinical use could be repurposed for RA, a disease that affects tens of millions of people worldwide.</p><p>We studied three health insurance databases: PearlDiver Mariner (2010–2021), IBM Marketscan Research Databases (2006–2020), and Veterans Administration (VA) Health database (2001–2021) (Supporting Information: Tables S1–S4). Inclusion criteria were at least 6 months follow-up, at least 18 years of age, schizophrenia or Tourette disorder diagnosed on two separate occasions, and treatment with antipsychotics. RA before diagnosis of schizophrenia or Tourette disorder was exclusionary (Supporting Information: Figure S1). Disease claims were identified by ICD-9-CM and ICD-10-CM codes. Drug exposure was determined by prescriptions for generic or brand versions. Time from first prescription of antipsychotics to diagnosis of RA was the dependent variable. Sensitivity analyses were performed using diagnosis of schizophrenia or Tourette disorder as the index date and flagging treatment with antipsychotics within 60 days of schizophrenia or Tourette disorder diagnosis. Patients were censored when they developed RA, unenrolled, died, or switched between study medication groups. Cox proportional hazards regression analyses were performed to estimate the hazard of RA in relation to haloperidol use. We performed propensity score matching to create cohorts with similar baseline characteristics, reducing possible bias in estimating treatment effects. Additionally, to control for any residual covariate imbalance, we adjusted for RA-associated confounders: age, sex, smoking, body mass index, Charlson comorbidity index, and database entry year. Fine-Gray subdistribution hazard ratios for competing risk of mortality, corrected for covariates, were calculated for the VA, which contains mortality data. We performed inverse-variance weighted meta-analyses to estimate the combined hazard ratio (HR) and 95% confidence intervals (CI) using a random-effects model, computed prediction intervals, and Kaplan–Meier survival analyses.</p><p>The adjusted Cox proportional hazards regression models in the propensity-score-matched populations showed a protective association of haloperidol use against incident RA in each of the three databases (Figure 1A,B). The meta-analyses identified a protective effect of haloperidol in the main (pooled adjusted hazard ratio [aHR] = 0.69; 95% CI: 0.61–0.79; <i>p</i> = 0.0001) and sensitivity analyses (pooled aHR = 0.69; 95% CI: 0.58–0.81; <i>p</i> < 0.0001) (Figure 1A,B). The 95% prediction intervals for the hazard ratio, which provide insights into the range of outcomes in a hypothetical future study, were <1.0 in both analyses (Figure 1A,B), implying a future clinical trial would be estimated to have a >95% probability of identifying a protective effect. Subdistribution hazard ratios, accounting for the competing risk of mortality, in the VA revealed a protective effect (main analysis: aHR = 0.52; 95% CI: 0.27–0.98; <i>p</i> = 0.0002; sensitivity analysis: aHR = 0.48; 95% CI: 0.30–0.76; <i>p</i> = 0.0002). Kaplan–Meier survival analyses revealed that haloperidol use was associated with a lower risk of incident RA in all three databases in both analyses (Figure 1C,D).</p><p>We identified a significant association between haloperidol use and incident RA. Strengths of our study include replication in three cohorts that comprise most United States adults, adjustment for confounders, and propensity score matching, which simulates randomization and increases its validity. As this retrospective study was not randomized, there could be residual confounding or selection bias.</p><p>Haloperidol is reported to inhibit the cytokines interleukin-1β (IL-1β), IL-6, and tumor necrosis factor-α,<span><sup>3, 4</sup></span> which are known drivers of RA.<span><sup>5</sup></span> Dendritic cells and T helper 1 lymphocytes play crucial roles in the pathogenesis of RA.<span><sup>6</sup></span> Haloperidol suppresses the maturation and priming of these cells, respectively.<span><sup>7</sup></span> Together, such effects could, in part, underlie the mechanistic basis of how haloperidol exposure reduces the development of RA. Clinical studies in individuals with mental illness may face ethical challenges as well as recruitment challenges owing to the incidence in this population. However, taken together with the anti-inflammatory effects of haloperidol, our findings, which suggest a potential benefit of haloperidol in RA, provide a rationale for randomized controlled trials in a general population at risk for RA. Such prospective trials could provide causal insights.</p><p><b>Vidya L. Ambati</b>: Conceptualization (equal); data curation (equal); formal analysis (equal); funding acquisition (equal); methodology (equal); writing—original draft (equal); writing—review & editing (equal). <b>Tammy H. Cummings</b>: Methodology (equal); writing—review and editing (equal). <b>Praveen Yerramothu</b>: Data curation (equal); writing—review and editing (equal). <b>Joseph Nguyen</b>: Data curation (equal); writing—review and editing. <b>S. Scott Sutton</b>: Data curation (equal); funding acquisition; methodology (equal); writing—original draft (equal); writing—review and editing. <b>Brian C. Werner</b>: Conceptualization (equal); data curation (equal); funding acquisition; methodology (equal); supervision (equal); writing—original draft (equal); writing—review and editing. <b>Joseph Magagnoli</b>: Conceptualization (equal); data curation (equal); formal analysis (equal); funding acquisition; methodology (equal); supervision (equal); writing—original draft (equal); writing—review and editing (equal). All authors have read and approved the final manuscript.</p><p>S. Scott Sutton has received research grants from Boehringer Ingelheim, Coherus BioSciences, EMD Serono, and Alexion Pharmaceuticals, all for projects unrelated to study. Brian C. Werner and Vidya L. Ambati are named as inventors on matter-related patent applications filed by their university.</p><p>PearlDiver Mariner and IBM Marketscan Research Databases contained deidentified data deemed exempt by the University of Virginia Institutional Review Board (IRB). Veterans Administration (VA) Health database data analysis was compliant with Department of Veterans Affairs requirements and received IRB (1139248-1) and Research and Development Approval.</p>\",\"PeriodicalId\":74135,\"journal\":{\"name\":\"MedComm - Future medicine\",\"volume\":\"2 4\",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-11-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/mef2.66\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"MedComm - Future medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/mef2.66\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"MedComm - Future medicine","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/mef2.66","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
一个未控制的病例系列报道了氟哌啶醇治疗类风湿性关节炎(RA)的益处FDA不良事件报告系统的一项研究报告称,在RA患者中,使用氟哌啶醇等抗精神病药物的患者较少,并得出结论,抗精神病药物可以降低RA的发生风险。2然而,这些结果仅表明相反的情况:RA与使用抗精神病药物的风险降低有关;它们并没有表明抗精神病药物可以降低类风湿性关节炎的风险。同样的研究还检查了日本的一个小型雇员保险数据库,并报告了类风湿性关节炎和抗精神病药物(包括氟哌啶醇)之间的逆时间关系。这两项研究的局限性包括规模小、未经验证和不完整的记录、缺乏对社会人口学或临床混杂因素的纠正、处方的时间趋势变化以及选择性随访缺失。因此,我们试图进行一项强有力的药物流行病学研究,以确定氟哌啶醇(一种fda批准的用于治疗精神分裂症或图雷特症的药物)是否会影响三个大型全国性健康保险数据库(包括大多数美国人口)中发生RA的风险。我们这样做的目的是确定一种已经在临床使用的廉价药物是否可以重新用于治疗风湿性关节炎,这种疾病影响着全世界数千万人。我们研究了三个健康保险数据库:PearlDiver Mariner(2010-2021)、IBM Marketscan Research数据库(2006-2020)和退伍军人管理局(VA)健康数据库(2001-2021)(支持信息:表S1-S4)。纳入标准为随访至少6个月,年龄至少18岁,两次被诊断为精神分裂症或图雷特障碍,并接受抗精神病药物治疗。在诊断为精神分裂症或图雷特障碍之前,RA被排除在外(支持信息:图S1)。疾病索赔通过ICD-9-CM和ICD-10-CM代码进行识别。药物暴露是由仿制药或品牌药的处方决定的。从第一次开抗精神病药到诊断为类风湿性关节炎的时间是因变量。以精神分裂症或抽动秽语症的诊断为指标日期,并在精神分裂症或抽动秽语症诊断后60天内使用抗精神病药物进行敏感性分析。当患者出现类风湿关节炎、未登记、死亡或在研究药物组之间切换时,他们将被审查。采用Cox比例风险回归分析来估计与氟哌啶醇使用相关的RA风险。我们进行倾向评分匹配,以创建具有相似基线特征的队列,减少估计治疗效果时可能出现的偏差。此外,为了控制任何残留的协变量不平衡,我们调整了ra相关的混杂因素:年龄、性别、吸烟、体重指数、Charlson合并症指数和数据库输入年份。对包含死亡率数据的VA计算了经过协变量校正的竞争死亡率风险的细灰色亚分布风险比。我们使用随机效应模型、计算预测区间和Kaplan-Meier生存分析进行了反方差加权荟萃分析,以估计联合风险比(HR)和95%置信区间(CI)。在倾向评分匹配的人群中,调整后的Cox比例风险回归模型显示,在三个数据库中,氟哌啶醇的使用对RA的发生率都有保护作用(图1A,B)。荟萃分析确定氟哌啶醇对主要患者有保护作用(合并校正风险比[aHR] = 0.69;95% ci: 0.61-0.79;p = 0.0001)和敏感性分析(合并aHR = 0.69;95% ci: 0.58-0.81;p < 0.0001)(图1A,B)。在两项分析中,风险比的95%预测区间为1.0(图1A,B),这意味着未来的临床试验估计有95%的概率确定保护作用。风险比提供了对假设的未来研究结果范围的见解。考虑竞争死亡风险的亚分布风险比在VA中显示出保护作用(主要分析:aHR = 0.52;95% ci: 0.27-0.98;p = 0.0002;敏感性分析:aHR = 0.48;95% ci: 0.30-0.76;p = 0.0002)。Kaplan-Meier生存分析显示,在两个分析的所有三个数据库中,氟哌啶醇的使用与发生RA的风险较低相关(图1C,D)。我们发现氟哌啶醇的使用与RA的发生有显著的关联。我们研究的优势包括在包括大多数美国成年人的三个队列中进行复制,对混杂因素进行调整,以及倾向评分匹配,这模拟了随机化并提高了其有效性。由于这项回顾性研究不是随机的,因此可能存在残留的混杂或选择偏倚。 据报道,氟哌啶醇可抑制已知的ra驱动因子白细胞介素-1β (IL-1β)、IL-6和肿瘤坏死因子-α 3,4。5树突状细胞和T辅助淋巴细胞在ra的发病机制中起关键作用。6氟哌啶醇分别抑制这些细胞的成熟和启动总之,这些影响可能在一定程度上揭示了氟哌啶醇暴露如何减少类风湿关节炎发展的机制基础。精神疾病患者的临床研究可能面临伦理挑战以及由于这一人群的发病率而带来的招募挑战。然而,结合氟哌啶醇的抗炎作用,我们的研究结果表明氟哌啶醇对类风湿关节炎有潜在的益处,为在类风湿关节炎风险人群中进行随机对照试验提供了依据。这样的前瞻性试验可以提供因果关系的见解。Vidya L. Ambati:概念化(平等);数据管理(相等);形式分析(相等);获得资金(相等);方法(平等);写作-原稿(同等);writing-review,编辑(平等)。Tammy H. Cummings:方法论(相等);写作—评审与编辑(同等)。Praveen Yerramothu:数据管理(平等);写作—评审与编辑(同等)。Joseph Nguyen:数据管理(equal);写作-审查和编辑。S. Scott Sutton:数据管理(平等);资金收购;方法(平等);写作-原稿(同等);写作-审查和编辑。Brian C. Werner:概念化(平等);数据管理(相等);资金收购;方法(平等);监督(平等);写作-原稿(同等);写作-审查和编辑。Joseph Magagnoli:概念化(平等);数据管理(相等);形式分析(相等);资金收购;方法(平等);监督(平等);写作-原稿(同等);写作—评审与编辑(同等)。所有作者都已阅读并批准了定稿。Scott Sutton已经获得了Boehringer Ingelheim, Coherus BioSciences, EMD Serono和Alexion Pharmaceuticals的研究资助,这些项目都与研究无关。Brian C. Werner和Vidya L. Ambati在他们的大学提交的物质相关专利申请中被命名为发明家。PearlDiver Mariner和IBM Marketscan研究数据库包含弗吉尼亚大学机构审查委员会(IRB)认为豁免的未识别数据。退伍军人管理局(VA)的健康数据库数据分析符合退伍军人事务部的要求,并获得了IRB(1139248-1)和研发批准。
Association between haloperidol use and risk of rheumatoid arthritis
An uncontrolled case-series reported a benefit of haloperidol in rheumatoid arthritis (RA).1 A study of the FDA Adverse Events Reporting System reported that among RA patients there were fewer users of antipsychotic drugs, including haloperidol, and concluded that antipsychotic drugs could reduce the risk of developing RA.2 However, these results only suggest the converse: that RA is associated with a reduced risk of antipsychotic use; they do not indicate that antipsychotics reduce the risk of RA. The same study also examined a small employee insurance database in Japan and reported an inverse temporal relationship between RA and antipsychotic drugs, including haloperidol. Limitations of these two studies include small size, unverified and incomplete records, lack of correction for sociodemographic or clinical confounders, changing time-trends in prescriptions, and selective loss to follow-up. Therefore, we sought to undertake a robust pharmacoepidemiologic study of whether haloperidol, an FDA-approved drug for the treatment of schizophrenia or Tourette disorder, affects the risk of incident RA in three large nationwide health insurance databases that comprise most of the United States population. We did so with the goal of determining whether an inexpensive drug already in clinical use could be repurposed for RA, a disease that affects tens of millions of people worldwide.
We studied three health insurance databases: PearlDiver Mariner (2010–2021), IBM Marketscan Research Databases (2006–2020), and Veterans Administration (VA) Health database (2001–2021) (Supporting Information: Tables S1–S4). Inclusion criteria were at least 6 months follow-up, at least 18 years of age, schizophrenia or Tourette disorder diagnosed on two separate occasions, and treatment with antipsychotics. RA before diagnosis of schizophrenia or Tourette disorder was exclusionary (Supporting Information: Figure S1). Disease claims were identified by ICD-9-CM and ICD-10-CM codes. Drug exposure was determined by prescriptions for generic or brand versions. Time from first prescription of antipsychotics to diagnosis of RA was the dependent variable. Sensitivity analyses were performed using diagnosis of schizophrenia or Tourette disorder as the index date and flagging treatment with antipsychotics within 60 days of schizophrenia or Tourette disorder diagnosis. Patients were censored when they developed RA, unenrolled, died, or switched between study medication groups. Cox proportional hazards regression analyses were performed to estimate the hazard of RA in relation to haloperidol use. We performed propensity score matching to create cohorts with similar baseline characteristics, reducing possible bias in estimating treatment effects. Additionally, to control for any residual covariate imbalance, we adjusted for RA-associated confounders: age, sex, smoking, body mass index, Charlson comorbidity index, and database entry year. Fine-Gray subdistribution hazard ratios for competing risk of mortality, corrected for covariates, were calculated for the VA, which contains mortality data. We performed inverse-variance weighted meta-analyses to estimate the combined hazard ratio (HR) and 95% confidence intervals (CI) using a random-effects model, computed prediction intervals, and Kaplan–Meier survival analyses.
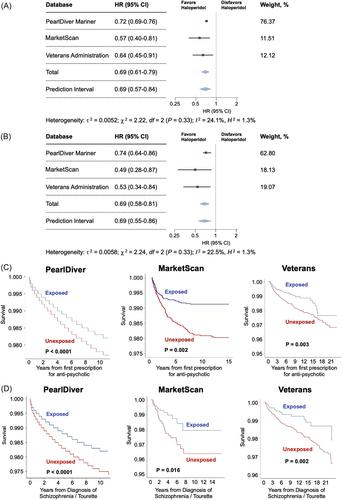
The adjusted Cox proportional hazards regression models in the propensity-score-matched populations showed a protective association of haloperidol use against incident RA in each of the three databases (Figure 1A,B). The meta-analyses identified a protective effect of haloperidol in the main (pooled adjusted hazard ratio [aHR] = 0.69; 95% CI: 0.61–0.79; p = 0.0001) and sensitivity analyses (pooled aHR = 0.69; 95% CI: 0.58–0.81; p < 0.0001) (Figure 1A,B). The 95% prediction intervals for the hazard ratio, which provide insights into the range of outcomes in a hypothetical future study, were <1.0 in both analyses (Figure 1A,B), implying a future clinical trial would be estimated to have a >95% probability of identifying a protective effect. Subdistribution hazard ratios, accounting for the competing risk of mortality, in the VA revealed a protective effect (main analysis: aHR = 0.52; 95% CI: 0.27–0.98; p = 0.0002; sensitivity analysis: aHR = 0.48; 95% CI: 0.30–0.76; p = 0.0002). Kaplan–Meier survival analyses revealed that haloperidol use was associated with a lower risk of incident RA in all three databases in both analyses (Figure 1C,D).
We identified a significant association between haloperidol use and incident RA. Strengths of our study include replication in three cohorts that comprise most United States adults, adjustment for confounders, and propensity score matching, which simulates randomization and increases its validity. As this retrospective study was not randomized, there could be residual confounding or selection bias.
Haloperidol is reported to inhibit the cytokines interleukin-1β (IL-1β), IL-6, and tumor necrosis factor-α,3, 4 which are known drivers of RA.5 Dendritic cells and T helper 1 lymphocytes play crucial roles in the pathogenesis of RA.6 Haloperidol suppresses the maturation and priming of these cells, respectively.7 Together, such effects could, in part, underlie the mechanistic basis of how haloperidol exposure reduces the development of RA. Clinical studies in individuals with mental illness may face ethical challenges as well as recruitment challenges owing to the incidence in this population. However, taken together with the anti-inflammatory effects of haloperidol, our findings, which suggest a potential benefit of haloperidol in RA, provide a rationale for randomized controlled trials in a general population at risk for RA. Such prospective trials could provide causal insights.
Vidya L. Ambati: Conceptualization (equal); data curation (equal); formal analysis (equal); funding acquisition (equal); methodology (equal); writing—original draft (equal); writing—review & editing (equal). Tammy H. Cummings: Methodology (equal); writing—review and editing (equal). Praveen Yerramothu: Data curation (equal); writing—review and editing (equal). Joseph Nguyen: Data curation (equal); writing—review and editing. S. Scott Sutton: Data curation (equal); funding acquisition; methodology (equal); writing—original draft (equal); writing—review and editing. Brian C. Werner: Conceptualization (equal); data curation (equal); funding acquisition; methodology (equal); supervision (equal); writing—original draft (equal); writing—review and editing. Joseph Magagnoli: Conceptualization (equal); data curation (equal); formal analysis (equal); funding acquisition; methodology (equal); supervision (equal); writing—original draft (equal); writing—review and editing (equal). All authors have read and approved the final manuscript.
S. Scott Sutton has received research grants from Boehringer Ingelheim, Coherus BioSciences, EMD Serono, and Alexion Pharmaceuticals, all for projects unrelated to study. Brian C. Werner and Vidya L. Ambati are named as inventors on matter-related patent applications filed by their university.
PearlDiver Mariner and IBM Marketscan Research Databases contained deidentified data deemed exempt by the University of Virginia Institutional Review Board (IRB). Veterans Administration (VA) Health database data analysis was compliant with Department of Veterans Affairs requirements and received IRB (1139248-1) and Research and Development Approval.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


