Kine Eide Kvitne, Markus Hovd, Line Kristin Johnson, Christine Wegler, Cecilia Karlsson, Per Artursson, Shalini Andersson, Rune Sandbu, Jøran Hjelmesæth, Eva Skovlund, Rasmus Jansson-Löfmark, Hege Christensen, Anders Åsberg, Ida Robertsen
{"title":"肥胖患者胃分流术前后或严格饮食与正常体重患者的地高辛药代动力学比较","authors":"Kine Eide Kvitne, Markus Hovd, Line Kristin Johnson, Christine Wegler, Cecilia Karlsson, Per Artursson, Shalini Andersson, Rune Sandbu, Jøran Hjelmesæth, Eva Skovlund, Rasmus Jansson-Löfmark, Hege Christensen, Anders Åsberg, Ida Robertsen","doi":"10.1007/s40262-023-01320-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objective: </strong>Several drugs on the market are substrates for P-glycoprotein (P-gp), an efflux transporter highly expressed in barrier tissues such as the intestine. Body weight, weight loss, and a Roux-en-Y gastric bypass (RYGB) may influence P-gp expression and activity, leading to variability in the drug response. The objective of this study was therefore to investigate digoxin pharmacokinetics as a measure of the P-gp phenotype in patients with obesity before and after weight loss induced by an RYGB or a strict diet and in normal weight individuals.</p><p><strong>Methods: </strong>This study included patients with severe obesity preparing for an RYGB (n = 40) or diet-induced weight loss (n = 40) and mainly normal weight individuals scheduled for a cholecystectomy (n = 18). Both weight loss groups underwent a 3-week low-energy diet (<1200 kcal/day) followed by an additional 6 weeks of <800 kcal/day induced by an RYGB (performed at week 3) or a very-low-energy diet. Follow-up time was 2 years, with four digoxin pharmacokinetic investigations at weeks 0, 3, and 9, and year 2. Hepatic and jejunal P-gp levels were determined in biopsies obtained from the patients undergoing surgery.</p><p><strong>Results: </strong>The RYGB group and the diet group had a comparable weight loss in the first 9 weeks (13 ± 2.3% and 11 ± 3.6%, respectively). During this period, we observed a minor increase (16%) in the digoxin area under the concentration-time curve from zero to infinity in both groups: RYGB: 2.7 µg h/L [95% confidence interval (CI) 0.67, 4.7], diet: 2.5 µg h/L [95% CI 0.49, 4.4]. In the RYGB group, we also observed that the time to reach maximum concentration decreased after surgery: from 1.0 ± 0.33 hours at week 3 to 0.77 ± 0.08 hours at week 9 (-0.26 hours [95% CI -0.47, -0.05]), corresponding to a 25% reduction. Area under the concentration-time curve from zero to infinity did not change long term (week 0 to year 2) in either the RYGB (1.1 µg h/L [-0.94, 3.2]) or the diet group (0.94 µg h/L [-1.2, 3.0]), despite a considerable difference in weight loss from baseline (RYGB: 30 ± 7%, diet: 3 ± 6%). At baseline, the area under the concentration-time curve from zero to infinity was -5.5 µg h/L [95% CI -8.5, -2.5] (-26%) lower in patients with obesity (RYGB plus diet) than in normal weight individuals scheduled for a cholecystectomy. Further, patients undergoing an RYGB had a 0.05 fmol/µg [95% CI 0.00, 0.10] (29%) higher hepatic P-gp level than the normal weight individuals.</p><p><strong>Conclusions: </strong>Changes in digoxin pharmacokinetics following weight loss induced by a pre-operative low-energy diet and an RYGB or a strict diet (a low-energy diet plus a very-low-energy diet) were minor and unlikely to be clinically relevant. The lower systemic exposure of digoxin in patients with obesity suggests that these patients may have increased biliary excretion of digoxin possibly owing to a higher expression of P-gp in the liver.</p>","PeriodicalId":10405,"journal":{"name":"Clinical Pharmacokinetics","volume":null,"pages":null},"PeriodicalIF":4.6000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10786955/pdf/","citationCount":"0","resultStr":"{\"title\":\"Digoxin Pharmacokinetics in Patients with Obesity Before and After a Gastric Bypass or a Strict Diet Compared with Normal Weight Individuals.\",\"authors\":\"Kine Eide Kvitne, Markus Hovd, Line Kristin Johnson, Christine Wegler, Cecilia Karlsson, Per Artursson, Shalini Andersson, Rune Sandbu, Jøran Hjelmesæth, Eva Skovlund, Rasmus Jansson-Löfmark, Hege Christensen, Anders Åsberg, Ida Robertsen\",\"doi\":\"10.1007/s40262-023-01320-9\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and objective: </strong>Several drugs on the market are substrates for P-glycoprotein (P-gp), an efflux transporter highly expressed in barrier tissues such as the intestine. Body weight, weight loss, and a Roux-en-Y gastric bypass (RYGB) may influence P-gp expression and activity, leading to variability in the drug response. The objective of this study was therefore to investigate digoxin pharmacokinetics as a measure of the P-gp phenotype in patients with obesity before and after weight loss induced by an RYGB or a strict diet and in normal weight individuals.</p><p><strong>Methods: </strong>This study included patients with severe obesity preparing for an RYGB (n = 40) or diet-induced weight loss (n = 40) and mainly normal weight individuals scheduled for a cholecystectomy (n = 18). Both weight loss groups underwent a 3-week low-energy diet (<1200 kcal/day) followed by an additional 6 weeks of <800 kcal/day induced by an RYGB (performed at week 3) or a very-low-energy diet. Follow-up time was 2 years, with four digoxin pharmacokinetic investigations at weeks 0, 3, and 9, and year 2. Hepatic and jejunal P-gp levels were determined in biopsies obtained from the patients undergoing surgery.</p><p><strong>Results: </strong>The RYGB group and the diet group had a comparable weight loss in the first 9 weeks (13 ± 2.3% and 11 ± 3.6%, respectively). During this period, we observed a minor increase (16%) in the digoxin area under the concentration-time curve from zero to infinity in both groups: RYGB: 2.7 µg h/L [95% confidence interval (CI) 0.67, 4.7], diet: 2.5 µg h/L [95% CI 0.49, 4.4]. In the RYGB group, we also observed that the time to reach maximum concentration decreased after surgery: from 1.0 ± 0.33 hours at week 3 to 0.77 ± 0.08 hours at week 9 (-0.26 hours [95% CI -0.47, -0.05]), corresponding to a 25% reduction. Area under the concentration-time curve from zero to infinity did not change long term (week 0 to year 2) in either the RYGB (1.1 µg h/L [-0.94, 3.2]) or the diet group (0.94 µg h/L [-1.2, 3.0]), despite a considerable difference in weight loss from baseline (RYGB: 30 ± 7%, diet: 3 ± 6%). At baseline, the area under the concentration-time curve from zero to infinity was -5.5 µg h/L [95% CI -8.5, -2.5] (-26%) lower in patients with obesity (RYGB plus diet) than in normal weight individuals scheduled for a cholecystectomy. Further, patients undergoing an RYGB had a 0.05 fmol/µg [95% CI 0.00, 0.10] (29%) higher hepatic P-gp level than the normal weight individuals.</p><p><strong>Conclusions: </strong>Changes in digoxin pharmacokinetics following weight loss induced by a pre-operative low-energy diet and an RYGB or a strict diet (a low-energy diet plus a very-low-energy diet) were minor and unlikely to be clinically relevant. The lower systemic exposure of digoxin in patients with obesity suggests that these patients may have increased biliary excretion of digoxin possibly owing to a higher expression of P-gp in the liver.</p>\",\"PeriodicalId\":10405,\"journal\":{\"name\":\"Clinical Pharmacokinetics\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":4.6000,\"publicationDate\":\"2024-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10786955/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Pharmacokinetics\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s40262-023-01320-9\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/11/22 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Pharmacokinetics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40262-023-01320-9","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/11/22 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
摘要
背景和目的:市场上的几种药物是p -糖蛋白(P-gp)的底物,p -糖蛋白是一种在肠等屏障组织中高度表达的外排转运蛋白。体重、体重减轻和Roux-en-Y胃旁路术(RYGB)可能影响P-gp的表达和活性,导致药物反应的变异性。因此,本研究的目的是研究地高辛药代动力学在RYGB或严格饮食引起的体重减轻前后和正常体重的肥胖患者中作为P-gp表型的测量指标。方法:本研究包括准备RYGB的严重肥胖患者(n = 40)或饮食引起的减肥患者(n = 40),以及主要是计划进行胆囊切除术的正常体重患者(n = 18)。两个减肥组都进行了为期3周的低能量饮食(结果:RYGB组和饮食组在前9周的体重减轻幅度相当(分别为13±2.3%和11±3.6%)。在此期间,我们观察到两组地高辛在浓度-时间曲线下从零到无穷大的面积都有小幅增加(16%):RYGB: 2.7µg h/L[95%置信区间(CI) 0.67, 4.7],日粮:2.5µg h/L [95% CI 0.49, 4.4]。在RYGB组中,我们还观察到手术后达到最大浓度的时间缩短:从第3周的1.0±0.33小时减少到第9周的0.77±0.08小时(-0.26小时[95% CI -0.47, -0.05]),相当于减少了25%。在RYGB组(1.1µg h/L[-0.94, 3.2])和饮食组(0.94µg h/L[-1.2, 3.0])中,从零到无限的浓度-时间曲线下的面积长期(第0周到第2年)没有变化,尽管与基线相比体重减轻有很大差异(RYGB组:30±7%,饮食组:3±6%)。在基线时,肥胖患者(RYGB加饮食)的浓度-时间曲线下的面积从0到无穷远为-5.5µg h/L [95% CI -8.5, -2.5](-26%)低于计划进行胆囊切除术的正常体重患者。此外,接受RYGB的患者肝脏P-gp水平比正常体重个体高0.05 fmol/µg [95% CI 0.00, 0.10](29%)。结论:术前低能量饮食和RYGB或严格饮食(低能量饮食加极低能量饮食)引起的体重减轻后地高辛药代动力学的变化很小,不太可能与临床相关。肥胖患者地高辛的低系统性暴露表明,这些患者可能由于肝脏中P-gp的高表达而增加了地高辛的胆汁排泄。
Digoxin Pharmacokinetics in Patients with Obesity Before and After a Gastric Bypass or a Strict Diet Compared with Normal Weight Individuals.
Background and objective: Several drugs on the market are substrates for P-glycoprotein (P-gp), an efflux transporter highly expressed in barrier tissues such as the intestine. Body weight, weight loss, and a Roux-en-Y gastric bypass (RYGB) may influence P-gp expression and activity, leading to variability in the drug response. The objective of this study was therefore to investigate digoxin pharmacokinetics as a measure of the P-gp phenotype in patients with obesity before and after weight loss induced by an RYGB or a strict diet and in normal weight individuals.
Methods: This study included patients with severe obesity preparing for an RYGB (n = 40) or diet-induced weight loss (n = 40) and mainly normal weight individuals scheduled for a cholecystectomy (n = 18). Both weight loss groups underwent a 3-week low-energy diet (<1200 kcal/day) followed by an additional 6 weeks of <800 kcal/day induced by an RYGB (performed at week 3) or a very-low-energy diet. Follow-up time was 2 years, with four digoxin pharmacokinetic investigations at weeks 0, 3, and 9, and year 2. Hepatic and jejunal P-gp levels were determined in biopsies obtained from the patients undergoing surgery.
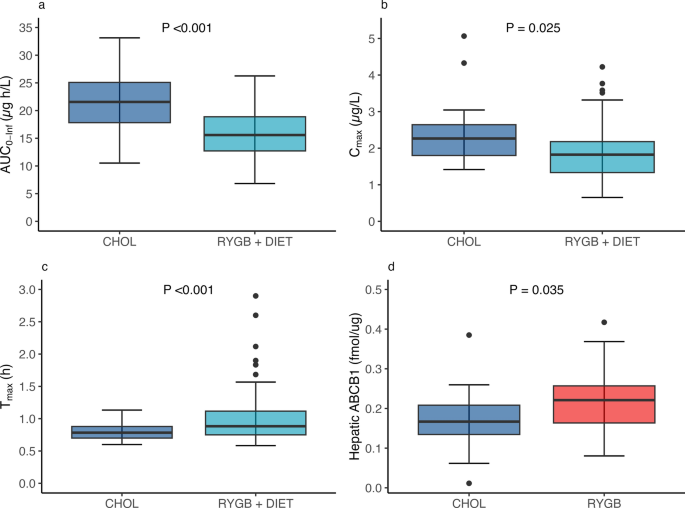
Results: The RYGB group and the diet group had a comparable weight loss in the first 9 weeks (13 ± 2.3% and 11 ± 3.6%, respectively). During this period, we observed a minor increase (16%) in the digoxin area under the concentration-time curve from zero to infinity in both groups: RYGB: 2.7 µg h/L [95% confidence interval (CI) 0.67, 4.7], diet: 2.5 µg h/L [95% CI 0.49, 4.4]. In the RYGB group, we also observed that the time to reach maximum concentration decreased after surgery: from 1.0 ± 0.33 hours at week 3 to 0.77 ± 0.08 hours at week 9 (-0.26 hours [95% CI -0.47, -0.05]), corresponding to a 25% reduction. Area under the concentration-time curve from zero to infinity did not change long term (week 0 to year 2) in either the RYGB (1.1 µg h/L [-0.94, 3.2]) or the diet group (0.94 µg h/L [-1.2, 3.0]), despite a considerable difference in weight loss from baseline (RYGB: 30 ± 7%, diet: 3 ± 6%). At baseline, the area under the concentration-time curve from zero to infinity was -5.5 µg h/L [95% CI -8.5, -2.5] (-26%) lower in patients with obesity (RYGB plus diet) than in normal weight individuals scheduled for a cholecystectomy. Further, patients undergoing an RYGB had a 0.05 fmol/µg [95% CI 0.00, 0.10] (29%) higher hepatic P-gp level than the normal weight individuals.
Conclusions: Changes in digoxin pharmacokinetics following weight loss induced by a pre-operative low-energy diet and an RYGB or a strict diet (a low-energy diet plus a very-low-energy diet) were minor and unlikely to be clinically relevant. The lower systemic exposure of digoxin in patients with obesity suggests that these patients may have increased biliary excretion of digoxin possibly owing to a higher expression of P-gp in the liver.
期刊介绍:
Clinical Pharmacokinetics promotes the continuing development of clinical pharmacokinetics and pharmacodynamics for the improvement of drug therapy, and for furthering postgraduate education in clinical pharmacology and therapeutics.
Pharmacokinetics, the study of drug disposition in the body, is an integral part of drug development and rational use. Knowledge and application of pharmacokinetic principles leads to accelerated drug development, cost effective drug use and a reduced frequency of adverse effects and drug interactions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


