Sithabisile Gugulethu Gigaba, Zamasomi Luvuno, Arvin Bhana, Andre Janse van Rensburg, Londiwe Mthethwa, Deepa Rao, Nikiwe Hongo, Inge Petersen
{"title":"在学习型医疗系统方法中利用质量改进,合作实施以证据为基础的综合初级精神保健一揽子计划:南非心理健康一体化计划的经验教训","authors":"Sithabisile Gugulethu Gigaba, Zamasomi Luvuno, Arvin Bhana, Andre Janse van Rensburg, Londiwe Mthethwa, Deepa Rao, Nikiwe Hongo, Inge Petersen","doi":"10.1002/lrh2.10389","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Introduction</h3>\n \n <p>The treatment gap for mental health disorders persists in low- and middle-income countries despite overwhelming evidence of the efficacy of task-sharing mental health interventions. Key barriers in the uptake of these innovations include the absence of policy to support implementation and diverting of staff from usual routines in health systems that are already overstretched. South Africa enjoys a conducive policy environment; however, strategies for operationalizing the policy ideals are lacking. This paper describes the Mental health INTegration Programme (MhINT), which adopted a health system strengthening approach to embed an evidence-based task-sharing care package for depression to integrate mental health care into chronic care at primary health care (PHC).</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>The MhINT care package consisting of psycho-education talks, nurse-led mental health assessment, and a structured psychosocial counselling intervention provided by lay counsellors was implemented in Amajuba district in KwaZulu-Natal over a 2-year period. A learning health systems approach was adopted, using continuous quality improvement (CQI) strategies to facilitate embedding of the intervention.</p>\n \n <p>MhINT was implemented along five phases: the project phase wherein teams to drive implementation were formed; the diagnostic phase where routinely collected data were used to identify system barriers to integrated mental health care; the intervention phase consisting of capacity building and using Plan-Do-Study-Act cycles to address implementation barriers and the impact and sustaining improvement phases entailed assessing the impact of the program and initiation of system-level interventions to sustain and institutionalize successful change ideas.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Integrated planning and monitoring were enabled by including key mental health service indicators in weekly meetings designed to track the performance of noncommunicable diseases and human immunovirus clinical programmes. Lack of standardization in mental health screening prompted the validation of a mental health screening tool and testing feasibility of its use in centralized screening stations. A culture of collaborative problem-solving was promoted through CQI data-driven learning sessions. The province-level screening rate increased by 10%, whilst the district screening rate increased by 7% and new patients initiated to mental health treatment increased by 16%.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>The CQI approach holds promise in facilitating the attainment of integrated mental health care in resource-scarce contexts. A collaborative relationship between researchers and health system stakeholders is an important strategy for facilitating the uptake of evidence-based innovations. However, the lack of interventions to address healthcare workers' own mental health poses a threat to integrated mental health care at PHC.</p>\n </section>\n </div>","PeriodicalId":43916,"journal":{"name":"Learning Health Systems","volume":"8 2","pages":""},"PeriodicalIF":2.6000,"publicationDate":"2023-10-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/lrh2.10389","citationCount":"0","resultStr":"{\"title\":\"Collaborative implementation of an evidence-based package of integrated primary mental healthcare using quality improvement within a learning health systems approach: Lessons from the Mental health INTegration programme in South Africa\",\"authors\":\"Sithabisile Gugulethu Gigaba, Zamasomi Luvuno, Arvin Bhana, Andre Janse van Rensburg, Londiwe Mthethwa, Deepa Rao, Nikiwe Hongo, Inge Petersen\",\"doi\":\"10.1002/lrh2.10389\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Introduction</h3>\\n \\n <p>The treatment gap for mental health disorders persists in low- and middle-income countries despite overwhelming evidence of the efficacy of task-sharing mental health interventions. Key barriers in the uptake of these innovations include the absence of policy to support implementation and diverting of staff from usual routines in health systems that are already overstretched. South Africa enjoys a conducive policy environment; however, strategies for operationalizing the policy ideals are lacking. This paper describes the Mental health INTegration Programme (MhINT), which adopted a health system strengthening approach to embed an evidence-based task-sharing care package for depression to integrate mental health care into chronic care at primary health care (PHC).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>The MhINT care package consisting of psycho-education talks, nurse-led mental health assessment, and a structured psychosocial counselling intervention provided by lay counsellors was implemented in Amajuba district in KwaZulu-Natal over a 2-year period. A learning health systems approach was adopted, using continuous quality improvement (CQI) strategies to facilitate embedding of the intervention.</p>\\n \\n <p>MhINT was implemented along five phases: the project phase wherein teams to drive implementation were formed; the diagnostic phase where routinely collected data were used to identify system barriers to integrated mental health care; the intervention phase consisting of capacity building and using Plan-Do-Study-Act cycles to address implementation barriers and the impact and sustaining improvement phases entailed assessing the impact of the program and initiation of system-level interventions to sustain and institutionalize successful change ideas.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Integrated planning and monitoring were enabled by including key mental health service indicators in weekly meetings designed to track the performance of noncommunicable diseases and human immunovirus clinical programmes. Lack of standardization in mental health screening prompted the validation of a mental health screening tool and testing feasibility of its use in centralized screening stations. A culture of collaborative problem-solving was promoted through CQI data-driven learning sessions. The province-level screening rate increased by 10%, whilst the district screening rate increased by 7% and new patients initiated to mental health treatment increased by 16%.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>The CQI approach holds promise in facilitating the attainment of integrated mental health care in resource-scarce contexts. A collaborative relationship between researchers and health system stakeholders is an important strategy for facilitating the uptake of evidence-based innovations. However, the lack of interventions to address healthcare workers' own mental health poses a threat to integrated mental health care at PHC.</p>\\n </section>\\n </div>\",\"PeriodicalId\":43916,\"journal\":{\"name\":\"Learning Health Systems\",\"volume\":\"8 2\",\"pages\":\"\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2023-10-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/lrh2.10389\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Learning Health Systems\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/lrh2.10389\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"HEALTH POLICY & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Learning Health Systems","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/lrh2.10389","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEALTH POLICY & SERVICES","Score":null,"Total":0}
Collaborative implementation of an evidence-based package of integrated primary mental healthcare using quality improvement within a learning health systems approach: Lessons from the Mental health INTegration programme in South Africa
Introduction
The treatment gap for mental health disorders persists in low- and middle-income countries despite overwhelming evidence of the efficacy of task-sharing mental health interventions. Key barriers in the uptake of these innovations include the absence of policy to support implementation and diverting of staff from usual routines in health systems that are already overstretched. South Africa enjoys a conducive policy environment; however, strategies for operationalizing the policy ideals are lacking. This paper describes the Mental health INTegration Programme (MhINT), which adopted a health system strengthening approach to embed an evidence-based task-sharing care package for depression to integrate mental health care into chronic care at primary health care (PHC).
Methods
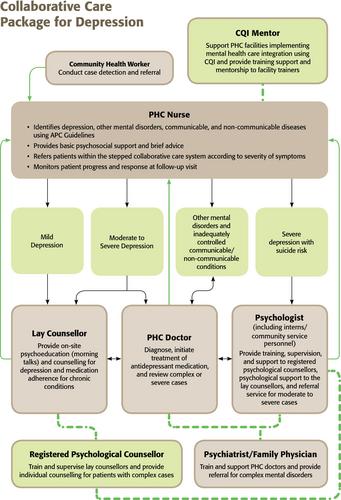
The MhINT care package consisting of psycho-education talks, nurse-led mental health assessment, and a structured psychosocial counselling intervention provided by lay counsellors was implemented in Amajuba district in KwaZulu-Natal over a 2-year period. A learning health systems approach was adopted, using continuous quality improvement (CQI) strategies to facilitate embedding of the intervention.
MhINT was implemented along five phases: the project phase wherein teams to drive implementation were formed; the diagnostic phase where routinely collected data were used to identify system barriers to integrated mental health care; the intervention phase consisting of capacity building and using Plan-Do-Study-Act cycles to address implementation barriers and the impact and sustaining improvement phases entailed assessing the impact of the program and initiation of system-level interventions to sustain and institutionalize successful change ideas.
Results
Integrated planning and monitoring were enabled by including key mental health service indicators in weekly meetings designed to track the performance of noncommunicable diseases and human immunovirus clinical programmes. Lack of standardization in mental health screening prompted the validation of a mental health screening tool and testing feasibility of its use in centralized screening stations. A culture of collaborative problem-solving was promoted through CQI data-driven learning sessions. The province-level screening rate increased by 10%, whilst the district screening rate increased by 7% and new patients initiated to mental health treatment increased by 16%.
Conclusions
The CQI approach holds promise in facilitating the attainment of integrated mental health care in resource-scarce contexts. A collaborative relationship between researchers and health system stakeholders is an important strategy for facilitating the uptake of evidence-based innovations. However, the lack of interventions to address healthcare workers' own mental health poses a threat to integrated mental health care at PHC.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


