{"title":"玛丽-约瑟夫修女结节","authors":"Zi Qin Ng, Adrian Teo, Tim Mitchell","doi":"10.1002/aid2.13381","DOIUrl":null,"url":null,"abstract":"<p>A 75-year-old male was referred for investigation of a painless, erythematous umbilical nodule that had been increasing in size for several months. The lesion was 2.5 cm in diameter, with an irregular border and superficial ulceration (Figure 1A). He had a recent admission for cholangitis secondary to choledocholithiasis but was otherwise feeling well. His past medical history was significant for ischemic heart disease with cardiac stents, and alcohol-related cirrhosis with portal hypertension. Given concern for a primary gastrointestinal malignancy, he proceeded to endoscopy. This demonstrated two small (10–15 mm), superficial antral ulcers (Figure 1B). These were confirmed on biopsy to be poorly differentiated gastric adenocarcinoma. Staging CT chest, abdomen, and pelvis did not show any distant metastases (Figure 2A). A diagnostic laparoscopy was performed and excluded peritoneal disease. The umbilical nodule was excised to assist with staging. Unexpectedly, histology showed that the umbilical nodule was a metastasis from prostate adenocarcinoma. This was confirmed on the immunohistochemistry staining which showed tumor cell expression with prostate-specific antigen and prostate-specific acid phosphatase.</p><p>PET (68 PSMA-11) imaging (Figure 2B) confirmed metastatic prostate cancer with disease in mediastinal lymph nodes, axial skeleton, and left lung. His case was discussed in the multidisciplinary meeting. Due to his frailty and co-morbidities, he underwent endoscopic submucosal dissection of the gastric adenocarcinoma. The histopathology showed two foci of poorly differentiated gastric adenocarcinoma (9 and 12 mm) invading the muscularis mucosae (pT1a). There was no lymphovascular invasion and the margins (lateral and deep) were negative. The metastatic prostate cancer was treated with palliative radiotherapy to deposits in T11 and L4, as well as androgen deprivation therapy. Further systemic therapy was not administered due to his co-morbidities. His disease is stable, and the patient continues to live independently 18 months later.</p><p>Sister Mary Joseph nodule represents a cutaneous metastasis, most commonly from the gastrointestinal tract. It is uncommon finding, occurring in up to 3% of abdominal and pelvic malignancies.<span><sup>1</sup></span> It is extremely rare for prostate cancer to cause a Sister Mary Joseph nodule, with only a few cases reported.<span><sup>2</sup></span> Appearance is variable and clinicians should demonstrate a high index of suspicion to avoid misdiagnosis.<span><sup>1, 2</sup></span> Histological sampling is vital as identification of the primary tumor may be difficult, as demonstrated by this case. Accurate disease staging is necessary for appropriate treatment.</p><p><b>Zi Qin Ng:</b> Study design, data collection and analysis, drafting of manuscript. <b>Adrian Teo:</b> Performed the surgery, and Review of the manuscript. <b>Tim Mitchell:</b> Data collection and analysis, critical review of manuscript.</p><p>The authors declare no conflicts of interest.</p><p>The patient has provided consent for the submission and publication of this manuscript.</p>","PeriodicalId":7278,"journal":{"name":"Advances in Digestive Medicine","volume":"11 2","pages":"105-106"},"PeriodicalIF":0.4000,"publicationDate":"2023-11-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/aid2.13381","citationCount":"0","resultStr":"{\"title\":\"Sister Mary Joseph nodule\",\"authors\":\"Zi Qin Ng, Adrian Teo, Tim Mitchell\",\"doi\":\"10.1002/aid2.13381\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>A 75-year-old male was referred for investigation of a painless, erythematous umbilical nodule that had been increasing in size for several months. The lesion was 2.5 cm in diameter, with an irregular border and superficial ulceration (Figure 1A). He had a recent admission for cholangitis secondary to choledocholithiasis but was otherwise feeling well. His past medical history was significant for ischemic heart disease with cardiac stents, and alcohol-related cirrhosis with portal hypertension. Given concern for a primary gastrointestinal malignancy, he proceeded to endoscopy. This demonstrated two small (10–15 mm), superficial antral ulcers (Figure 1B). These were confirmed on biopsy to be poorly differentiated gastric adenocarcinoma. Staging CT chest, abdomen, and pelvis did not show any distant metastases (Figure 2A). A diagnostic laparoscopy was performed and excluded peritoneal disease. The umbilical nodule was excised to assist with staging. Unexpectedly, histology showed that the umbilical nodule was a metastasis from prostate adenocarcinoma. This was confirmed on the immunohistochemistry staining which showed tumor cell expression with prostate-specific antigen and prostate-specific acid phosphatase.</p><p>PET (68 PSMA-11) imaging (Figure 2B) confirmed metastatic prostate cancer with disease in mediastinal lymph nodes, axial skeleton, and left lung. His case was discussed in the multidisciplinary meeting. Due to his frailty and co-morbidities, he underwent endoscopic submucosal dissection of the gastric adenocarcinoma. The histopathology showed two foci of poorly differentiated gastric adenocarcinoma (9 and 12 mm) invading the muscularis mucosae (pT1a). There was no lymphovascular invasion and the margins (lateral and deep) were negative. The metastatic prostate cancer was treated with palliative radiotherapy to deposits in T11 and L4, as well as androgen deprivation therapy. Further systemic therapy was not administered due to his co-morbidities. His disease is stable, and the patient continues to live independently 18 months later.</p><p>Sister Mary Joseph nodule represents a cutaneous metastasis, most commonly from the gastrointestinal tract. It is uncommon finding, occurring in up to 3% of abdominal and pelvic malignancies.<span><sup>1</sup></span> It is extremely rare for prostate cancer to cause a Sister Mary Joseph nodule, with only a few cases reported.<span><sup>2</sup></span> Appearance is variable and clinicians should demonstrate a high index of suspicion to avoid misdiagnosis.<span><sup>1, 2</sup></span> Histological sampling is vital as identification of the primary tumor may be difficult, as demonstrated by this case. Accurate disease staging is necessary for appropriate treatment.</p><p><b>Zi Qin Ng:</b> Study design, data collection and analysis, drafting of manuscript. <b>Adrian Teo:</b> Performed the surgery, and Review of the manuscript. <b>Tim Mitchell:</b> Data collection and analysis, critical review of manuscript.</p><p>The authors declare no conflicts of interest.</p><p>The patient has provided consent for the submission and publication of this manuscript.</p>\",\"PeriodicalId\":7278,\"journal\":{\"name\":\"Advances in Digestive Medicine\",\"volume\":\"11 2\",\"pages\":\"105-106\"},\"PeriodicalIF\":0.4000,\"publicationDate\":\"2023-11-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/aid2.13381\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Advances in Digestive Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/aid2.13381\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advances in Digestive Medicine","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/aid2.13381","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
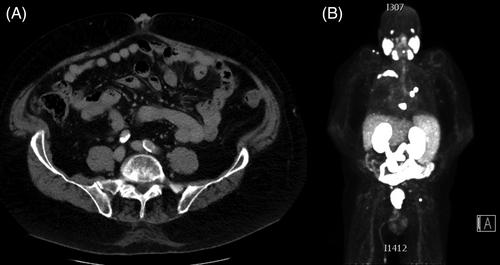
A 75-year-old male was referred for investigation of a painless, erythematous umbilical nodule that had been increasing in size for several months. The lesion was 2.5 cm in diameter, with an irregular border and superficial ulceration (Figure 1A). He had a recent admission for cholangitis secondary to choledocholithiasis but was otherwise feeling well. His past medical history was significant for ischemic heart disease with cardiac stents, and alcohol-related cirrhosis with portal hypertension. Given concern for a primary gastrointestinal malignancy, he proceeded to endoscopy. This demonstrated two small (10–15 mm), superficial antral ulcers (Figure 1B). These were confirmed on biopsy to be poorly differentiated gastric adenocarcinoma. Staging CT chest, abdomen, and pelvis did not show any distant metastases (Figure 2A). A diagnostic laparoscopy was performed and excluded peritoneal disease. The umbilical nodule was excised to assist with staging. Unexpectedly, histology showed that the umbilical nodule was a metastasis from prostate adenocarcinoma. This was confirmed on the immunohistochemistry staining which showed tumor cell expression with prostate-specific antigen and prostate-specific acid phosphatase.
PET (68 PSMA-11) imaging (Figure 2B) confirmed metastatic prostate cancer with disease in mediastinal lymph nodes, axial skeleton, and left lung. His case was discussed in the multidisciplinary meeting. Due to his frailty and co-morbidities, he underwent endoscopic submucosal dissection of the gastric adenocarcinoma. The histopathology showed two foci of poorly differentiated gastric adenocarcinoma (9 and 12 mm) invading the muscularis mucosae (pT1a). There was no lymphovascular invasion and the margins (lateral and deep) were negative. The metastatic prostate cancer was treated with palliative radiotherapy to deposits in T11 and L4, as well as androgen deprivation therapy. Further systemic therapy was not administered due to his co-morbidities. His disease is stable, and the patient continues to live independently 18 months later.
Sister Mary Joseph nodule represents a cutaneous metastasis, most commonly from the gastrointestinal tract. It is uncommon finding, occurring in up to 3% of abdominal and pelvic malignancies.1 It is extremely rare for prostate cancer to cause a Sister Mary Joseph nodule, with only a few cases reported.2 Appearance is variable and clinicians should demonstrate a high index of suspicion to avoid misdiagnosis.1, 2 Histological sampling is vital as identification of the primary tumor may be difficult, as demonstrated by this case. Accurate disease staging is necessary for appropriate treatment.
Zi Qin Ng: Study design, data collection and analysis, drafting of manuscript. Adrian Teo: Performed the surgery, and Review of the manuscript. Tim Mitchell: Data collection and analysis, critical review of manuscript.
The authors declare no conflicts of interest.
The patient has provided consent for the submission and publication of this manuscript.
期刊介绍:
Advances in Digestive Medicine is the official peer-reviewed journal of GEST, DEST and TASL. Missions of AIDM are to enhance the quality of patient care, to promote researches in gastroenterology, endoscopy and hepatology related fields, and to develop platforms for digestive science. Specific areas of interest are included, but not limited to: • Acid-related disease • Small intestinal disease • Digestive cancer • Diagnostic & therapeutic endoscopy • Enteral nutrition • Innovation in endoscopic technology • Functional GI • Hepatitis • GI images • Liver cirrhosis • Gut hormone • NASH • Helicobacter pylori • Cancer screening • IBD • Laparoscopic surgery • Infectious disease of digestive tract • Genetics and metabolic disorder • Microbiota • Regenerative medicine • Pancreaticobiliary disease • Guideline & consensus.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


