{"title":"肺炎高危患者拔管后微创造口术的疗效:一个病例系列。","authors":"Akira Ouchi, Yuji Takahashi, Hidehiko Nakano, Masaki Mochizuki, Saiko Okamoto, Hideaki Sakuramoto, Kensuke Nakamura","doi":"10.2478/jccm-2023-0029","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Minitracheostomy involves the percutaneous insertion of a 4-mm-diameter cricothyroidotomy tube for tracheal suctioning to facilitate the clearance of airway secretions. The advantage of using the minitracheostomy is in the clearance of secretions, however data on their usefulness for respiratory failure after extubation is limited. Aim of the study: We aimed to assess the use of minitracheostomy for patients with challenging extubation caused by significant sputum.</p><p><strong>Material and methods: </strong>We conducted a retrospective analysis of consecutive case series. We analyzed the data of 31 patients with pneumonia. After minitracheostomy, the primary endpoints of reintubation within 72 hours and clinical effects, including mortality, length of intensive care unit (ICU), or hospital stay, were assessed. The successful extubation group included patients who did not require reintubation within 72 hours. Conversely, the reintubation group consisted of patients mandating reestablishment of intubation within 72 hours.</p><p><strong>Results: </strong>Among those who underwent minitracheostomy after extubation, 22 (71%) underwent successful extubation and 9 underwent reintubation (reintubation rate: 29%). The in-hospital mortality rates after 30 days were 18.2% in the successful extubation group and 22.2% in the reintubation group. The ICU and hospital lengths of stay were 11 days (interquartile range: 8-14.3 days) and 23 days (interquartile range: 15.5-41 days), respectively, in the successful extubation group; they were 14 days (interquartile range: 11-18.5 days) and 30 days (interquartile range: 16-45.5 days), respectively, in the reintubation group.</p><p><strong>Conclusions: </strong>The prophylactic use of minitracheostomy may be an option as a means of reducing reintubation in patients with pneumonia who are at very high risk of reintubation.</p>","PeriodicalId":44227,"journal":{"name":"Journal of Critical Care Medicine","volume":"9 4","pages":"271-276"},"PeriodicalIF":1.7000,"publicationDate":"2023-11-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10644282/pdf/","citationCount":"0","resultStr":"{\"title\":\"Effectiveness of Minitracheostomy After Extubation in Patients with Pneumonia at High Risk of Reintubation: A Case Series.\",\"authors\":\"Akira Ouchi, Yuji Takahashi, Hidehiko Nakano, Masaki Mochizuki, Saiko Okamoto, Hideaki Sakuramoto, Kensuke Nakamura\",\"doi\":\"10.2478/jccm-2023-0029\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Minitracheostomy involves the percutaneous insertion of a 4-mm-diameter cricothyroidotomy tube for tracheal suctioning to facilitate the clearance of airway secretions. The advantage of using the minitracheostomy is in the clearance of secretions, however data on their usefulness for respiratory failure after extubation is limited. Aim of the study: We aimed to assess the use of minitracheostomy for patients with challenging extubation caused by significant sputum.</p><p><strong>Material and methods: </strong>We conducted a retrospective analysis of consecutive case series. We analyzed the data of 31 patients with pneumonia. After minitracheostomy, the primary endpoints of reintubation within 72 hours and clinical effects, including mortality, length of intensive care unit (ICU), or hospital stay, were assessed. The successful extubation group included patients who did not require reintubation within 72 hours. Conversely, the reintubation group consisted of patients mandating reestablishment of intubation within 72 hours.</p><p><strong>Results: </strong>Among those who underwent minitracheostomy after extubation, 22 (71%) underwent successful extubation and 9 underwent reintubation (reintubation rate: 29%). The in-hospital mortality rates after 30 days were 18.2% in the successful extubation group and 22.2% in the reintubation group. The ICU and hospital lengths of stay were 11 days (interquartile range: 8-14.3 days) and 23 days (interquartile range: 15.5-41 days), respectively, in the successful extubation group; they were 14 days (interquartile range: 11-18.5 days) and 30 days (interquartile range: 16-45.5 days), respectively, in the reintubation group.</p><p><strong>Conclusions: </strong>The prophylactic use of minitracheostomy may be an option as a means of reducing reintubation in patients with pneumonia who are at very high risk of reintubation.</p>\",\"PeriodicalId\":44227,\"journal\":{\"name\":\"Journal of Critical Care Medicine\",\"volume\":\"9 4\",\"pages\":\"271-276\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2023-11-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10644282/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Critical Care Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2478/jccm-2023-0029\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/10/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Critical Care Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2478/jccm-2023-0029","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/10/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
Effectiveness of Minitracheostomy After Extubation in Patients with Pneumonia at High Risk of Reintubation: A Case Series.
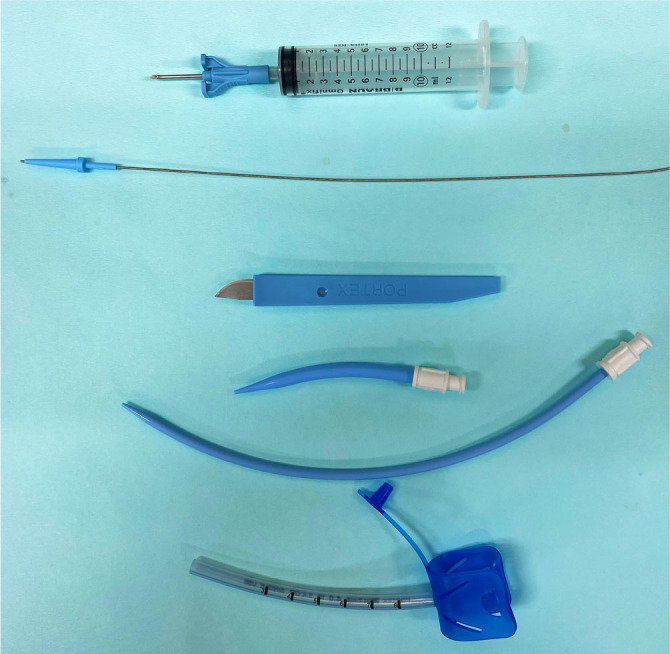
Introduction: Minitracheostomy involves the percutaneous insertion of a 4-mm-diameter cricothyroidotomy tube for tracheal suctioning to facilitate the clearance of airway secretions. The advantage of using the minitracheostomy is in the clearance of secretions, however data on their usefulness for respiratory failure after extubation is limited. Aim of the study: We aimed to assess the use of minitracheostomy for patients with challenging extubation caused by significant sputum.
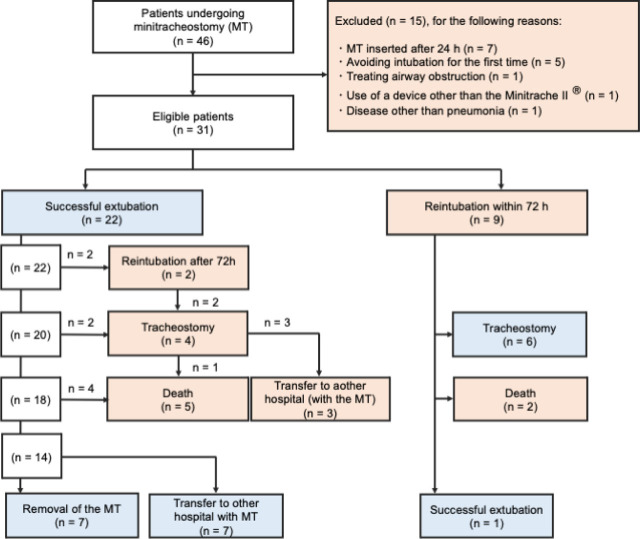
Material and methods: We conducted a retrospective analysis of consecutive case series. We analyzed the data of 31 patients with pneumonia. After minitracheostomy, the primary endpoints of reintubation within 72 hours and clinical effects, including mortality, length of intensive care unit (ICU), or hospital stay, were assessed. The successful extubation group included patients who did not require reintubation within 72 hours. Conversely, the reintubation group consisted of patients mandating reestablishment of intubation within 72 hours.
Results: Among those who underwent minitracheostomy after extubation, 22 (71%) underwent successful extubation and 9 underwent reintubation (reintubation rate: 29%). The in-hospital mortality rates after 30 days were 18.2% in the successful extubation group and 22.2% in the reintubation group. The ICU and hospital lengths of stay were 11 days (interquartile range: 8-14.3 days) and 23 days (interquartile range: 15.5-41 days), respectively, in the successful extubation group; they were 14 days (interquartile range: 11-18.5 days) and 30 days (interquartile range: 16-45.5 days), respectively, in the reintubation group.
Conclusions: The prophylactic use of minitracheostomy may be an option as a means of reducing reintubation in patients with pneumonia who are at very high risk of reintubation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


