Artemios G Karagiannidis, Maria-Eleni Alexandrou, George Lioulios, Maria Stangou, Pantelis A Sarafidis, Aikaterini Papagianni
{"title":"晚期慢性肾脏病伴危及生命的低钾血症,由未确诊的吉特曼综合征引起。","authors":"Artemios G Karagiannidis, Maria-Eleni Alexandrou, George Lioulios, Maria Stangou, Pantelis A Sarafidis, Aikaterini Papagianni","doi":"10.5414/CNCS110977","DOIUrl":null,"url":null,"abstract":"<p><p>We report a case of a 58-year-old woman presenting with symptoms of oliguria, fatigue, anorexia, constipation, hypovolemic signs, and laboratory tests showing severe hypokalemia (1.7 mEq/L), hyponatremia (120 mEq/L), high serum creatinine (SCr, 6.46 mg/dL) and urea (352 mg/dL). The patient had previously been diagnosed with chronic kidney disease (CKD), with SCr up to 2.58 mg/dL 1 year prior, and had in all her previous laboratory tests shown hypokalemia, which was treated with conservative measures and eplerenone despite low-normal blood pressure and normal heart function. A set of coordinated measures were applied to restore the potassium deficit, revert hypovolemic hyponatremia, and support renal function (including 4 dialysis sessions). In addition, a careful diagnostic approach revealed inappropriately high urine sodium and potassium losses, hypocalciuria, and hyperreninemic hyperaldosteronism leading to the diagnosis of Gitelman syndrome and hypokalemia-associated chronic tubulointerstitial nephropathy. Importantly, compliance with a simple set of instructions on high potassium and liberal sodium diet enabled the patient not only to remain euvolemic, free of symptoms, and with normal electrolytes, but also to recover a significant part of renal function and stabilize at an earlier CKD stage. Gitelman syndrome is a rare disorder that can be easily diagnosed and treated following simple measures; its early diagnosis is necessary to avoid life-threatening complications.</p>","PeriodicalId":10398,"journal":{"name":"Clinical Nephrology. Case Studies","volume":"11 ","pages":"22-28"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9948751/pdf/","citationCount":"0","resultStr":"{\"title\":\"Advanced chronic kidney disease with life-threatening hypokalemia due to undiagnosed Gitelman syndrome.\",\"authors\":\"Artemios G Karagiannidis, Maria-Eleni Alexandrou, George Lioulios, Maria Stangou, Pantelis A Sarafidis, Aikaterini Papagianni\",\"doi\":\"10.5414/CNCS110977\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>We report a case of a 58-year-old woman presenting with symptoms of oliguria, fatigue, anorexia, constipation, hypovolemic signs, and laboratory tests showing severe hypokalemia (1.7 mEq/L), hyponatremia (120 mEq/L), high serum creatinine (SCr, 6.46 mg/dL) and urea (352 mg/dL). The patient had previously been diagnosed with chronic kidney disease (CKD), with SCr up to 2.58 mg/dL 1 year prior, and had in all her previous laboratory tests shown hypokalemia, which was treated with conservative measures and eplerenone despite low-normal blood pressure and normal heart function. A set of coordinated measures were applied to restore the potassium deficit, revert hypovolemic hyponatremia, and support renal function (including 4 dialysis sessions). In addition, a careful diagnostic approach revealed inappropriately high urine sodium and potassium losses, hypocalciuria, and hyperreninemic hyperaldosteronism leading to the diagnosis of Gitelman syndrome and hypokalemia-associated chronic tubulointerstitial nephropathy. Importantly, compliance with a simple set of instructions on high potassium and liberal sodium diet enabled the patient not only to remain euvolemic, free of symptoms, and with normal electrolytes, but also to recover a significant part of renal function and stabilize at an earlier CKD stage. Gitelman syndrome is a rare disorder that can be easily diagnosed and treated following simple measures; its early diagnosis is necessary to avoid life-threatening complications.</p>\",\"PeriodicalId\":10398,\"journal\":{\"name\":\"Clinical Nephrology. Case Studies\",\"volume\":\"11 \",\"pages\":\"22-28\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9948751/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Nephrology. Case Studies\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5414/CNCS110977\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Nephrology. Case Studies","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5414/CNCS110977","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Advanced chronic kidney disease with life-threatening hypokalemia due to undiagnosed Gitelman syndrome.
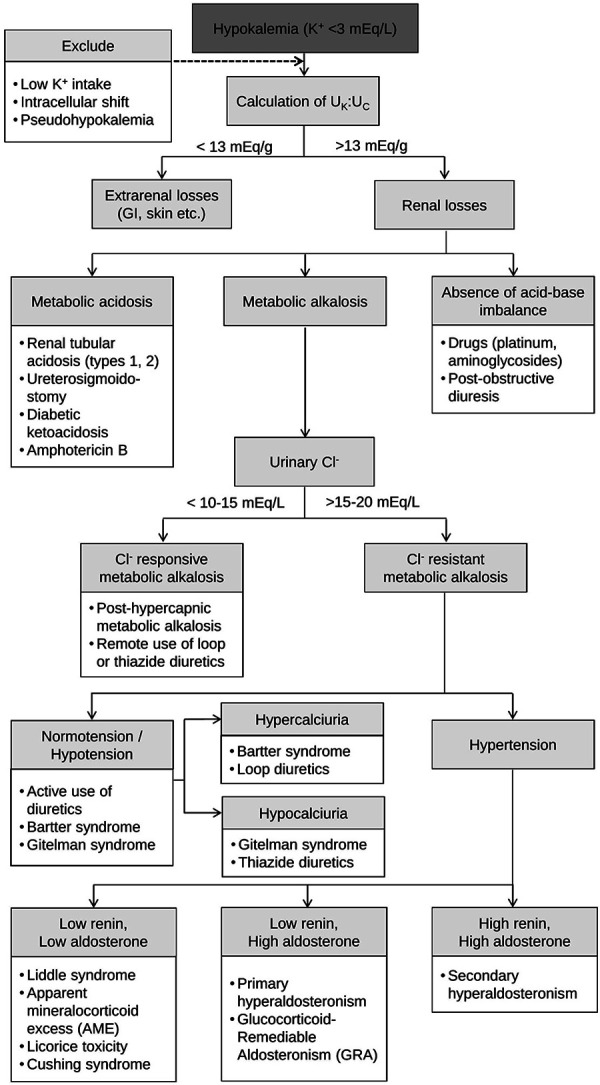
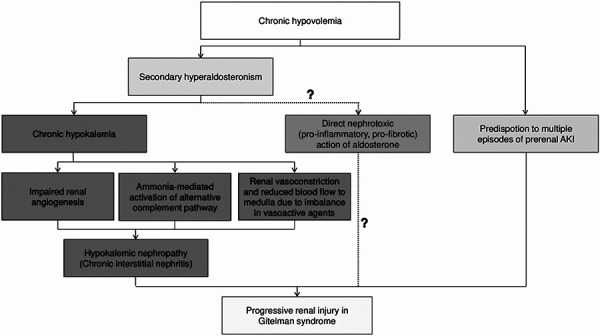
We report a case of a 58-year-old woman presenting with symptoms of oliguria, fatigue, anorexia, constipation, hypovolemic signs, and laboratory tests showing severe hypokalemia (1.7 mEq/L), hyponatremia (120 mEq/L), high serum creatinine (SCr, 6.46 mg/dL) and urea (352 mg/dL). The patient had previously been diagnosed with chronic kidney disease (CKD), with SCr up to 2.58 mg/dL 1 year prior, and had in all her previous laboratory tests shown hypokalemia, which was treated with conservative measures and eplerenone despite low-normal blood pressure and normal heart function. A set of coordinated measures were applied to restore the potassium deficit, revert hypovolemic hyponatremia, and support renal function (including 4 dialysis sessions). In addition, a careful diagnostic approach revealed inappropriately high urine sodium and potassium losses, hypocalciuria, and hyperreninemic hyperaldosteronism leading to the diagnosis of Gitelman syndrome and hypokalemia-associated chronic tubulointerstitial nephropathy. Importantly, compliance with a simple set of instructions on high potassium and liberal sodium diet enabled the patient not only to remain euvolemic, free of symptoms, and with normal electrolytes, but also to recover a significant part of renal function and stabilize at an earlier CKD stage. Gitelman syndrome is a rare disorder that can be easily diagnosed and treated following simple measures; its early diagnosis is necessary to avoid life-threatening complications.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


