Elisabeth M Jongbloed, Hedwig M Blommestein, Hannah M van Schoubroeck, John W M Martens, Saskia M Wilting, Carin A Uyl-de Groot, Agnes Jager
{"title":"Abemaciclib在早期乳腺癌患者中的成本-效果:一刀切还是根据患者需求量身定制?","authors":"Elisabeth M Jongbloed, Hedwig M Blommestein, Hannah M van Schoubroeck, John W M Martens, Saskia M Wilting, Carin A Uyl-de Groot, Agnes Jager","doi":"10.2147/BCTT.S387375","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>The addition of two years of abemaciclib treatment to standard adjuvant endocrine therapy in all patients with high risk ER+, HER2- early breast cancer (EBC) has been approved by the US Food and Drug Administration (FDA). Pre-selection of patients with an immediate risk of recurrence within the group of clinically high risk patients using detection of minimal residual disease (MRD) using patient-informed circulating tumor DNA assays during follow-up could enhance efficacy. Here, we investigate the cost-effectiveness of the addition of two years abemaciclib in all high risk HR+, HER2- patients and in MRD-guided high risk patients only.</p><p><strong>Methods: </strong>Two semi-Markov models were developed to evaluate the cost-effectiveness of adding two years of abemaciclib compared to \"standard treatment\": 1) \"abemaciclib all\" and 2) \"MRD-guided abemaciclib\" using MRD-guidance. Data of the MonarchE trial were used to model the invasive disease-free survival (iDFS). Since iDFS and overall survival (OS) data of abemaciclib were currently limited, abemaciclib effects were extrapolated using a favorable, intermediate and unfavorable effect scenario.</p><p><strong>Results: </strong>The addition of abemaciclib in all high-risk EBC patients prolonged iDFS slightly (0.04 additional quality adjusted life years (QALYs)) and led to higher costs compared to standard ET, leading to a high incremental cost effectiveness ratio (ICER) of €1,551,876/QALY. Neither the favorable effect scenario (additional 1.09 QALYs) was cost-effective (ICER €62,935/QALY), using a willingness-to-pay threshold of €50,000/QALY. The \"MRD-guided abemaciclib\" strategy resulted in lower costs and an increase in QALYs (1.27) compared to \"standard treatment\" in the unfavorable effect scenario.</p><p><strong>Conclusion: </strong>The addition of abemaciclib to adjuvant endocrine therapy in all high-risk ER+, HER2- EBC patients is not cost-effective. However, using MRD detection to justify the addition of abemaciclib treatment dominates standard treatment in this cost-effectiveness analysis. Further evaluation of MRD detection in EBC by means of prospective clinical trials assessing clinical utility is recommended and promising in terms of cost-effectiveness.</p>","PeriodicalId":72459,"journal":{"name":"","volume":"15 ","pages":"147-161"},"PeriodicalIF":0.0,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/53/f0/bctt-15-147.PMC9940501.pdf","citationCount":"0","resultStr":"{\"title\":\"Cost-Effectiveness of Abemaciclib in Early Breast Cancer Patients: One Size Fits All or Tailoring to Patients' Needs?\",\"authors\":\"Elisabeth M Jongbloed, Hedwig M Blommestein, Hannah M van Schoubroeck, John W M Martens, Saskia M Wilting, Carin A Uyl-de Groot, Agnes Jager\",\"doi\":\"10.2147/BCTT.S387375\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>The addition of two years of abemaciclib treatment to standard adjuvant endocrine therapy in all patients with high risk ER+, HER2- early breast cancer (EBC) has been approved by the US Food and Drug Administration (FDA). Pre-selection of patients with an immediate risk of recurrence within the group of clinically high risk patients using detection of minimal residual disease (MRD) using patient-informed circulating tumor DNA assays during follow-up could enhance efficacy. Here, we investigate the cost-effectiveness of the addition of two years abemaciclib in all high risk HR+, HER2- patients and in MRD-guided high risk patients only.</p><p><strong>Methods: </strong>Two semi-Markov models were developed to evaluate the cost-effectiveness of adding two years of abemaciclib compared to \\\"standard treatment\\\": 1) \\\"abemaciclib all\\\" and 2) \\\"MRD-guided abemaciclib\\\" using MRD-guidance. Data of the MonarchE trial were used to model the invasive disease-free survival (iDFS). Since iDFS and overall survival (OS) data of abemaciclib were currently limited, abemaciclib effects were extrapolated using a favorable, intermediate and unfavorable effect scenario.</p><p><strong>Results: </strong>The addition of abemaciclib in all high-risk EBC patients prolonged iDFS slightly (0.04 additional quality adjusted life years (QALYs)) and led to higher costs compared to standard ET, leading to a high incremental cost effectiveness ratio (ICER) of €1,551,876/QALY. Neither the favorable effect scenario (additional 1.09 QALYs) was cost-effective (ICER €62,935/QALY), using a willingness-to-pay threshold of €50,000/QALY. The \\\"MRD-guided abemaciclib\\\" strategy resulted in lower costs and an increase in QALYs (1.27) compared to \\\"standard treatment\\\" in the unfavorable effect scenario.</p><p><strong>Conclusion: </strong>The addition of abemaciclib to adjuvant endocrine therapy in all high-risk ER+, HER2- EBC patients is not cost-effective. However, using MRD detection to justify the addition of abemaciclib treatment dominates standard treatment in this cost-effectiveness analysis. Further evaluation of MRD detection in EBC by means of prospective clinical trials assessing clinical utility is recommended and promising in terms of cost-effectiveness.</p>\",\"PeriodicalId\":72459,\"journal\":{\"name\":\"\",\"volume\":\"15 \",\"pages\":\"147-161\"},\"PeriodicalIF\":0.0,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/53/f0/bctt-15-147.PMC9940501.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.2147/BCTT.S387375\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/BCTT.S387375","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Cost-Effectiveness of Abemaciclib in Early Breast Cancer Patients: One Size Fits All or Tailoring to Patients' Needs?
Purpose: The addition of two years of abemaciclib treatment to standard adjuvant endocrine therapy in all patients with high risk ER+, HER2- early breast cancer (EBC) has been approved by the US Food and Drug Administration (FDA). Pre-selection of patients with an immediate risk of recurrence within the group of clinically high risk patients using detection of minimal residual disease (MRD) using patient-informed circulating tumor DNA assays during follow-up could enhance efficacy. Here, we investigate the cost-effectiveness of the addition of two years abemaciclib in all high risk HR+, HER2- patients and in MRD-guided high risk patients only.
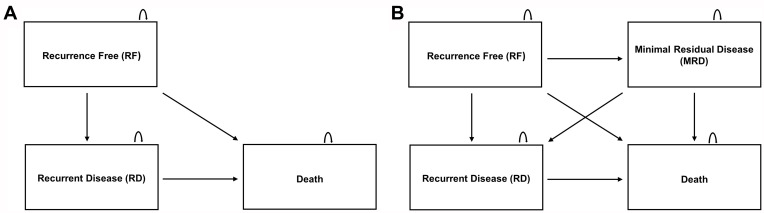
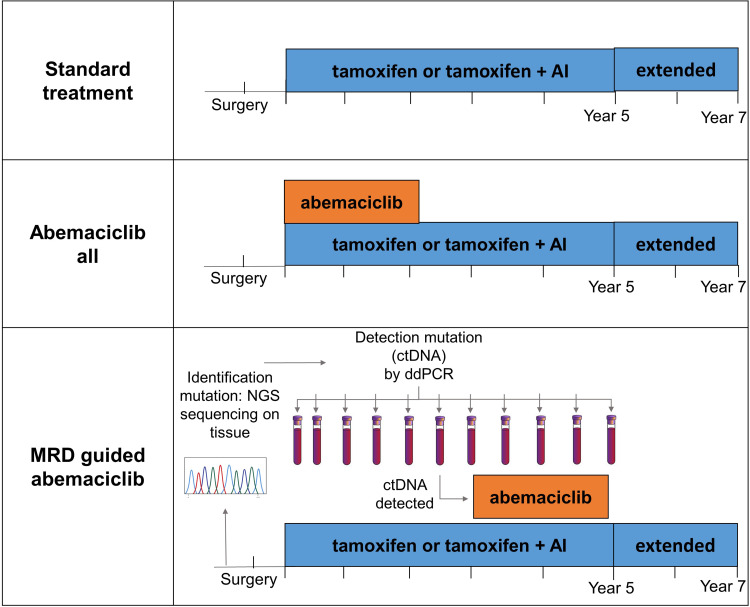
Methods: Two semi-Markov models were developed to evaluate the cost-effectiveness of adding two years of abemaciclib compared to "standard treatment": 1) "abemaciclib all" and 2) "MRD-guided abemaciclib" using MRD-guidance. Data of the MonarchE trial were used to model the invasive disease-free survival (iDFS). Since iDFS and overall survival (OS) data of abemaciclib were currently limited, abemaciclib effects were extrapolated using a favorable, intermediate and unfavorable effect scenario.
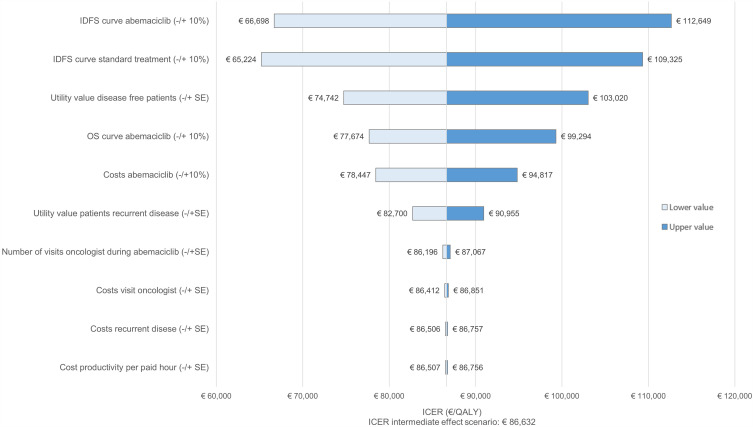
Results: The addition of abemaciclib in all high-risk EBC patients prolonged iDFS slightly (0.04 additional quality adjusted life years (QALYs)) and led to higher costs compared to standard ET, leading to a high incremental cost effectiveness ratio (ICER) of €1,551,876/QALY. Neither the favorable effect scenario (additional 1.09 QALYs) was cost-effective (ICER €62,935/QALY), using a willingness-to-pay threshold of €50,000/QALY. The "MRD-guided abemaciclib" strategy resulted in lower costs and an increase in QALYs (1.27) compared to "standard treatment" in the unfavorable effect scenario.
Conclusion: The addition of abemaciclib to adjuvant endocrine therapy in all high-risk ER+, HER2- EBC patients is not cost-effective. However, using MRD detection to justify the addition of abemaciclib treatment dominates standard treatment in this cost-effectiveness analysis. Further evaluation of MRD detection in EBC by means of prospective clinical trials assessing clinical utility is recommended and promising in terms of cost-effectiveness.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


