Evgeniya Shalaeva, Arjola Bano, Ulugbek Kasimov, Bakhtiyor Janabaev, Iris Baumgartner, Markus Laimer, Hugo Saner
{"title":"冠状动脉钙化评分和冠状动脉计算机断层扫描血管造影可预测接受部分截肢的 2 型糖尿病和外周动脉疾病患者的一年死亡率。","authors":"Evgeniya Shalaeva, Arjola Bano, Ulugbek Kasimov, Bakhtiyor Janabaev, Iris Baumgartner, Markus Laimer, Hugo Saner","doi":"10.1177/14791641221125190","DOIUrl":null,"url":null,"abstract":"<p><strong>Methods: </strong>This is a single-center prospective cohort study including 199 consecutive patients with T2D, PAD (mean age 62.3 ± 7.2 years; 62.8% males), and preoperative CACS and CCTA undergoing PFA and followed-up over 1 year.</p><p><strong>Results: </strong>Over a period of 1 year follow-up, a total of 35 (17.6%) participants died. The area under ROC curve to predict mortality for the CACS was 0.835 (95% CI:0.769-0.900), for CCTA 0.858 (95% CI:0.788-0.927). After adjustment for confounders, compared to no-stenosis on CCTA (reference), the risk of all-cause mortality in non-obstructive coronary atery disease (CAD) increased (HR = 1.38, 95% CI [0.75-12.86], <i>p</i> = .284), 1-vessel obstructive CAD (HR = 8.13, 95% CI [0.87-75.88], <i>p</i> = .066), 2-vessels (HR = 10.94, 95% CI [1.03-115.8], <i>p</i> = .047), and 3-vessels (HR = 45.73, 95% CI [4.6-454.7], <i>p</i> = .001) respectively. Increasing levels of CACS tended to be associated with increased risk of all-cause mortality (HR = 1.002, 95% CI [1.0-1.003], <i>p</i> = .061). 61/95 patients with obstructive CAD underwent coronary revascularization.</p><p><strong>Conclusions: </strong>Coronary artery calcium score and CCTA have a high predictive value for 1-year all-cause mortality in T2D patients undergoing minor amputations and may be considered for preoperative risk assessment allowing timely preventive interventions.</p>","PeriodicalId":11092,"journal":{"name":"Diabetes & Vascular Disease Research","volume":"19 5","pages":"14791641221125190"},"PeriodicalIF":3.0000,"publicationDate":"2022-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9558880/pdf/","citationCount":"0","resultStr":"{\"title\":\"Coronary artery calcium score and coronary computed tomography angiography predict one-year mortality in patients with type 2 diabetes and peripheral artery disease undergoing partial foot amputation.\",\"authors\":\"Evgeniya Shalaeva, Arjola Bano, Ulugbek Kasimov, Bakhtiyor Janabaev, Iris Baumgartner, Markus Laimer, Hugo Saner\",\"doi\":\"10.1177/14791641221125190\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Methods: </strong>This is a single-center prospective cohort study including 199 consecutive patients with T2D, PAD (mean age 62.3 ± 7.2 years; 62.8% males), and preoperative CACS and CCTA undergoing PFA and followed-up over 1 year.</p><p><strong>Results: </strong>Over a period of 1 year follow-up, a total of 35 (17.6%) participants died. The area under ROC curve to predict mortality for the CACS was 0.835 (95% CI:0.769-0.900), for CCTA 0.858 (95% CI:0.788-0.927). After adjustment for confounders, compared to no-stenosis on CCTA (reference), the risk of all-cause mortality in non-obstructive coronary atery disease (CAD) increased (HR = 1.38, 95% CI [0.75-12.86], <i>p</i> = .284), 1-vessel obstructive CAD (HR = 8.13, 95% CI [0.87-75.88], <i>p</i> = .066), 2-vessels (HR = 10.94, 95% CI [1.03-115.8], <i>p</i> = .047), and 3-vessels (HR = 45.73, 95% CI [4.6-454.7], <i>p</i> = .001) respectively. Increasing levels of CACS tended to be associated with increased risk of all-cause mortality (HR = 1.002, 95% CI [1.0-1.003], <i>p</i> = .061). 61/95 patients with obstructive CAD underwent coronary revascularization.</p><p><strong>Conclusions: </strong>Coronary artery calcium score and CCTA have a high predictive value for 1-year all-cause mortality in T2D patients undergoing minor amputations and may be considered for preoperative risk assessment allowing timely preventive interventions.</p>\",\"PeriodicalId\":11092,\"journal\":{\"name\":\"Diabetes & Vascular Disease Research\",\"volume\":\"19 5\",\"pages\":\"14791641221125190\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2022-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9558880/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Diabetes & Vascular Disease Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/14791641221125190\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Diabetes & Vascular Disease Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/14791641221125190","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
摘要
方法:这是一项单中心前瞻性队列研究,包括199名连续接受PFA手术的T2D和PAD患者(平均年龄62.3 ± 7.2岁;62.8%为男性),他们术前均接受了CACS和CCTA检查,随访时间为1年:结果:在为期一年的随访中,共有 35 人(17.6%)死亡。CACS预测死亡率的ROC曲线下面积为0.835(95% CI:0.769-0.900),CCTA为0.858(95% CI:0.788-0.927)。调整混杂因素后,与 CCTA 无狭窄(参考值)相比,非梗阻性冠状动脉疾病(CAD)的全因死亡风险增加(HR = 1.38,95% CI [0.75-12.86],P = .284),1-血管阻塞性 CAD(HR = 8.13,95% CI [0.87-75.88],p = .066),2-血管(HR = 10.94,95% CI [1.03-115.8],p = .047)和 3-血管(HR = 45.73,95% CI [4.6-454.7],p = .001)分别增加。CACS水平的增加往往与全因死亡风险的增加有关(HR = 1.002,95% CI [1.0-1.003],p = .061)。61/95的阻塞性CAD患者接受了冠状动脉血运重建:结论:冠状动脉钙化评分和 CCTA 对接受轻微截肢手术的 T2D 患者的 1 年全因死亡率具有很高的预测价值,可考虑用于术前风险评估,以便及时采取预防性干预措施。
Coronary artery calcium score and coronary computed tomography angiography predict one-year mortality in patients with type 2 diabetes and peripheral artery disease undergoing partial foot amputation.
Methods: This is a single-center prospective cohort study including 199 consecutive patients with T2D, PAD (mean age 62.3 ± 7.2 years; 62.8% males), and preoperative CACS and CCTA undergoing PFA and followed-up over 1 year.
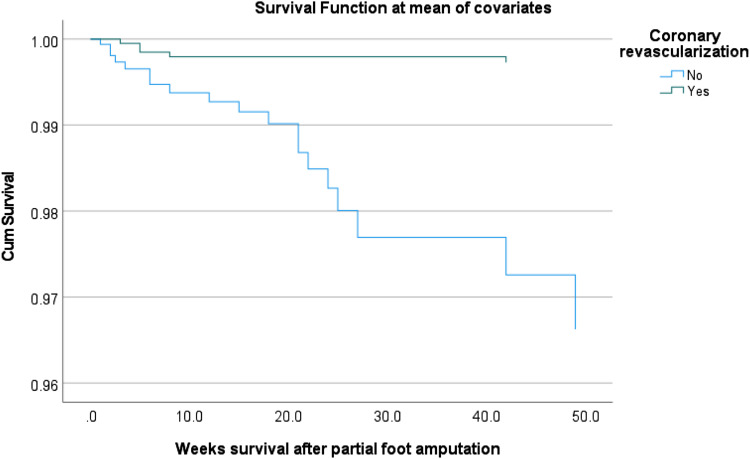
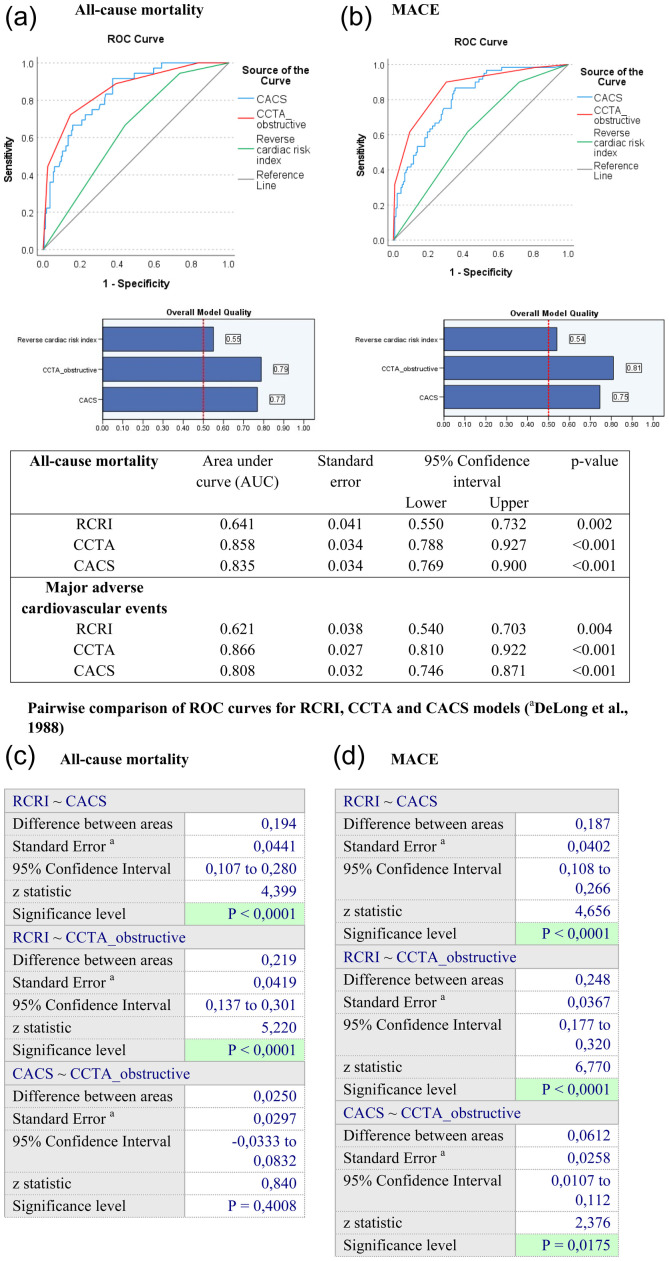
Results: Over a period of 1 year follow-up, a total of 35 (17.6%) participants died. The area under ROC curve to predict mortality for the CACS was 0.835 (95% CI:0.769-0.900), for CCTA 0.858 (95% CI:0.788-0.927). After adjustment for confounders, compared to no-stenosis on CCTA (reference), the risk of all-cause mortality in non-obstructive coronary atery disease (CAD) increased (HR = 1.38, 95% CI [0.75-12.86], p = .284), 1-vessel obstructive CAD (HR = 8.13, 95% CI [0.87-75.88], p = .066), 2-vessels (HR = 10.94, 95% CI [1.03-115.8], p = .047), and 3-vessels (HR = 45.73, 95% CI [4.6-454.7], p = .001) respectively. Increasing levels of CACS tended to be associated with increased risk of all-cause mortality (HR = 1.002, 95% CI [1.0-1.003], p = .061). 61/95 patients with obstructive CAD underwent coronary revascularization.
Conclusions: Coronary artery calcium score and CCTA have a high predictive value for 1-year all-cause mortality in T2D patients undergoing minor amputations and may be considered for preoperative risk assessment allowing timely preventive interventions.
期刊介绍:
Diabetes & Vascular Disease Research is the first international peer-reviewed journal to unite diabetes and vascular disease in a single title. The journal publishes original papers, research letters and reviews. This journal is a member of the Committee on Publication Ethics (COPE)


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


