{"title":"每日一次头孢曲松-阿米卡星联合用药作为经验性抗生素治疗,使儿童发热性中性粒细胞减少症的门诊管理成为可能——来自单一研究所的16年经验。","authors":"Shailesh Kanvinde, Atul Mulay, Anand Deshpande, Chetan Deshmukh, Sampada Patwardhan","doi":"10.1055/s-0042-1745834","DOIUrl":null,"url":null,"abstract":"<p><p>Shailesh Kanvinde<b>Background</b> To enable outpatient department (OPD) management of febrile neutropenia (FN), we used once-a-day (OD) ceftriaxone-amikacin (CFT-AMK) as empiric antibiotic therapy. Our experience over 16-year period is presented. <b>Methods</b> This was a retrospective study conducted from January2002 to December2017. Inclusion criteria were <18 years of age, undergoing cancer chemotherapy, and having FN. Exclusion criteria were FN after palliative chemotherapy, bone marrow transplantation, or at diagnosis of malignancy. Empiric CFT-AMK was used in all, except those having respiratory distress, hypotension, altered sensorium, paralytic ileus, or clinical evidence of peritonitis. Admission criteria were age <1 year, acute myeloid leukemia (AML) chemotherapy, poor performance status, need for blood transfusions, convenience, insurance, or persistent fever >48 to 72 hours after CFT-AMK. Outcomes analyzed were response (defervescence within 48-72 hours), OPD management, antibiotic upgrade, and mortality. AML diagnosis, >7 days to absolute neutrophil count >0.5 × 10 <sup>9</sup> /L, poor performance status, and malignancy not in remission were considered high-risk FN criteria. <b>Results</b> CFT-AMK was given in 877/952 (92.2%) FN episodes. Seventy-six percent had hematolymphoid malignancies. Response, antibiotic upgrade, and mortality were seen in 85.7 and 65.5% ( <i>p</i> < 0.0001), 15 and 45.5% ( <i>p</i> < 0.0001), and 0 and 2% ( <i>p</i> = 0.003) of low- and high-risk patients, respectively. Treatment was started in OPD in 52%, of which 21.6% required subsequent admission. Of those initially admitted, early discharge (hospital stay < 5 days) was possible in 24.6%. Forty-one percent episodes were managed entirely on OPD. Overall, 80% of low-risk and 42% of high-risk episodes received treatment wholly or partially on OPD. <b>Conclusion</b> Our results show empiric OD CFT-AMK allows OPD management for most of the low-risk and a proportion of high-risk FN following chemotherapy in children, without compromising clinical outcomes.</p>","PeriodicalId":22053,"journal":{"name":"South Asian Journal of Cancer","volume":"11 4","pages":"370-377"},"PeriodicalIF":0.8000,"publicationDate":"2022-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/8a/98/10-1055-s-0042-1745834.PMC9902091.pdf","citationCount":"0","resultStr":"{\"title\":\"Once-a-Day Ceftriaxone-Amikacin Combination as Empiric Antibiotic Therapy to Enable Outpatient Management of Febrile Neutropenia in Children-16-Year Experience from a Single Institute.\",\"authors\":\"Shailesh Kanvinde, Atul Mulay, Anand Deshpande, Chetan Deshmukh, Sampada Patwardhan\",\"doi\":\"10.1055/s-0042-1745834\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Shailesh Kanvinde<b>Background</b> To enable outpatient department (OPD) management of febrile neutropenia (FN), we used once-a-day (OD) ceftriaxone-amikacin (CFT-AMK) as empiric antibiotic therapy. Our experience over 16-year period is presented. <b>Methods</b> This was a retrospective study conducted from January2002 to December2017. Inclusion criteria were <18 years of age, undergoing cancer chemotherapy, and having FN. Exclusion criteria were FN after palliative chemotherapy, bone marrow transplantation, or at diagnosis of malignancy. Empiric CFT-AMK was used in all, except those having respiratory distress, hypotension, altered sensorium, paralytic ileus, or clinical evidence of peritonitis. Admission criteria were age <1 year, acute myeloid leukemia (AML) chemotherapy, poor performance status, need for blood transfusions, convenience, insurance, or persistent fever >48 to 72 hours after CFT-AMK. Outcomes analyzed were response (defervescence within 48-72 hours), OPD management, antibiotic upgrade, and mortality. AML diagnosis, >7 days to absolute neutrophil count >0.5 × 10 <sup>9</sup> /L, poor performance status, and malignancy not in remission were considered high-risk FN criteria. <b>Results</b> CFT-AMK was given in 877/952 (92.2%) FN episodes. Seventy-six percent had hematolymphoid malignancies. Response, antibiotic upgrade, and mortality were seen in 85.7 and 65.5% ( <i>p</i> < 0.0001), 15 and 45.5% ( <i>p</i> < 0.0001), and 0 and 2% ( <i>p</i> = 0.003) of low- and high-risk patients, respectively. Treatment was started in OPD in 52%, of which 21.6% required subsequent admission. Of those initially admitted, early discharge (hospital stay < 5 days) was possible in 24.6%. Forty-one percent episodes were managed entirely on OPD. Overall, 80% of low-risk and 42% of high-risk episodes received treatment wholly or partially on OPD. <b>Conclusion</b> Our results show empiric OD CFT-AMK allows OPD management for most of the low-risk and a proportion of high-risk FN following chemotherapy in children, without compromising clinical outcomes.</p>\",\"PeriodicalId\":22053,\"journal\":{\"name\":\"South Asian Journal of Cancer\",\"volume\":\"11 4\",\"pages\":\"370-377\"},\"PeriodicalIF\":0.8000,\"publicationDate\":\"2022-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/8a/98/10-1055-s-0042-1745834.PMC9902091.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"South Asian Journal of Cancer\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1055/s-0042-1745834\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"South Asian Journal of Cancer","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0042-1745834","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
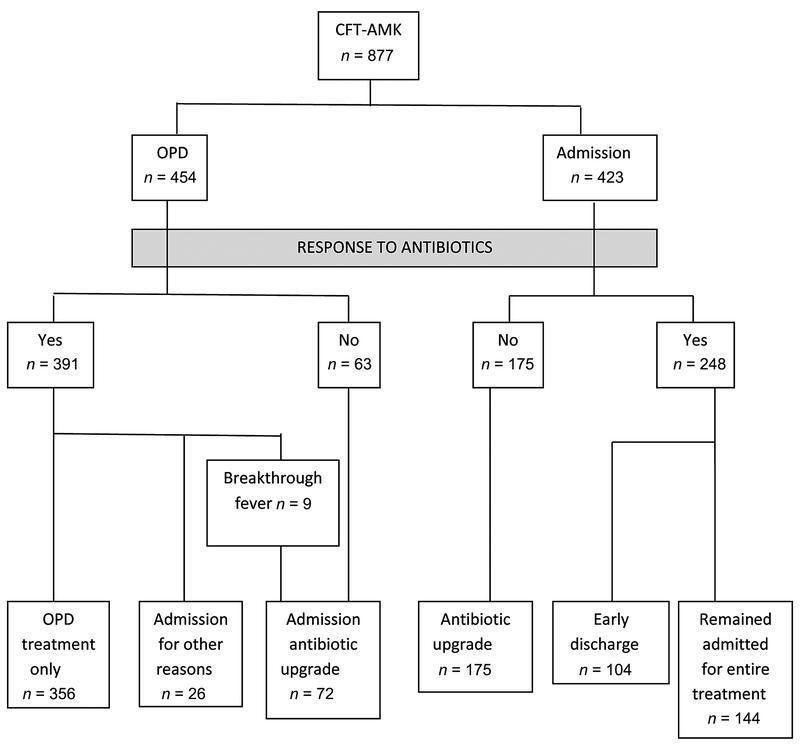
背景:为了使门诊(OPD)能够管理发热性中性粒细胞减少症(FN),我们使用一天一次(OD)头孢曲松-阿米卡星(CFT-AMK)作为经验性抗生素治疗。介绍了我们16年来的经验。方法回顾性研究时间为2002年1月至2017年12月。纳入标准为CFT-AMK后48 ~ 72小时。分析的结果包括反应(48-72小时内退热)、OPD管理、抗生素升级和死亡率。AML诊断,>7天到绝对中性粒细胞计数>0.5 × 10 9 /L,表现不佳,恶性肿瘤未缓解,被认为是高风险FN标准。结果877/952例FN发作(92.2%)给予CFT-AMK治疗。76%的人患有淋巴细胞恶性肿瘤。低危患者的反应、抗生素升级和死亡率分别为85.7和65.5% (p p p = 0.003)。52%的患者在门诊开始治疗,其中21.6%的患者需要后续入院。结论:我们的研究结果表明,经验性OD CFT-AMK可以对大多数低风险和一部分高风险的儿童化疗后FN进行OPD管理,而不会影响临床结果。
Once-a-Day Ceftriaxone-Amikacin Combination as Empiric Antibiotic Therapy to Enable Outpatient Management of Febrile Neutropenia in Children-16-Year Experience from a Single Institute.
Shailesh KanvindeBackground To enable outpatient department (OPD) management of febrile neutropenia (FN), we used once-a-day (OD) ceftriaxone-amikacin (CFT-AMK) as empiric antibiotic therapy. Our experience over 16-year period is presented. Methods This was a retrospective study conducted from January2002 to December2017. Inclusion criteria were <18 years of age, undergoing cancer chemotherapy, and having FN. Exclusion criteria were FN after palliative chemotherapy, bone marrow transplantation, or at diagnosis of malignancy. Empiric CFT-AMK was used in all, except those having respiratory distress, hypotension, altered sensorium, paralytic ileus, or clinical evidence of peritonitis. Admission criteria were age <1 year, acute myeloid leukemia (AML) chemotherapy, poor performance status, need for blood transfusions, convenience, insurance, or persistent fever >48 to 72 hours after CFT-AMK. Outcomes analyzed were response (defervescence within 48-72 hours), OPD management, antibiotic upgrade, and mortality. AML diagnosis, >7 days to absolute neutrophil count >0.5 × 10 9 /L, poor performance status, and malignancy not in remission were considered high-risk FN criteria. Results CFT-AMK was given in 877/952 (92.2%) FN episodes. Seventy-six percent had hematolymphoid malignancies. Response, antibiotic upgrade, and mortality were seen in 85.7 and 65.5% ( p < 0.0001), 15 and 45.5% ( p < 0.0001), and 0 and 2% ( p = 0.003) of low- and high-risk patients, respectively. Treatment was started in OPD in 52%, of which 21.6% required subsequent admission. Of those initially admitted, early discharge (hospital stay < 5 days) was possible in 24.6%. Forty-one percent episodes were managed entirely on OPD. Overall, 80% of low-risk and 42% of high-risk episodes received treatment wholly or partially on OPD. Conclusion Our results show empiric OD CFT-AMK allows OPD management for most of the low-risk and a proportion of high-risk FN following chemotherapy in children, without compromising clinical outcomes.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


