Felix Mensah, Joshua Okyere, Simon Agongo Azure, Eugene Budu, Edward Kwabena Ameyaw, Abdul-Aziz Seidu, Bright Opoku Ahinkorah
{"title":"避孕普及率方面的年龄、地理和社会经济不平等:1993-2014年加纳人口与健康调查的证据。","authors":"Felix Mensah, Joshua Okyere, Simon Agongo Azure, Eugene Budu, Edward Kwabena Ameyaw, Abdul-Aziz Seidu, Bright Opoku Ahinkorah","doi":"10.1186/s40834-022-00194-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Contraceptives afford individuals the opportunity to meet their reproductive needs and reduce maternal mortality. We aimed at assessing the trend and inequalities of contraceptive use in Ghana based on the 1993-2014 Ghana Demographic and Health Surveys.</p><p><strong>Methods: </strong>We used the World Health Organization's Health Equity Assessment Toolkit (HEAT) software in analysing the data. We adopted two approaches for the analysis. First, we disaggregated inequalities in contraceptive use using four equity stratifiers: wealth index, education, residence, and region. Second, summary measures (D), (PAR), (R), and (PAF) were also employed. A 95% uncertainty interval (UI) was constructed for point estimates to measure statistical significance.</p><p><strong>Results: </strong>Contraceptive prevalence increased from 20.3% in 1993 to 26.7% in 2014. The contraceptive prevalence among women aged 20-49 increased from 20.6% [95% UI = 19.1, 22.3] in 1993 to 26.8% [95% UI = 24.9, 28.9] in 2014 and this exceeded the increase that was recorded among those aged 15-19 (from 13% [95 UI = 8.7, 19] to 18% [95% UI = 11.5, 28.6]), in the same period. It was evident that substantial inequality existed with respect to contraceptive use, from 1993 to 2014, with widest inequality occurring in 2003 (PAF = 2.7, 95% UI = -16.6-21.9; D = 17.4, 95% UI = 12.7-22.1). In terms of wealth index, the least inequality was observed in 2014 (PAR = 1.3, 95% UI = -1-3.6; D = 5.9, 95% UI = -0.1-12). Regarding education, the widest inequality occurred in 1993 (PAF = 138.6, UI = 132.1-145.1; D = 40.1, 95% UI = 34.4-45.9). With place of residence, the widest gap in inequality occurred in 1993 (PAF = 51.2, 95% UI = 46.2-56.3; D = 15.3, 95% UI = 11.8-18.7). There was inequality in contraceptive use with respect to sub-national regions. In 2014, the Difference (D = 21, 95% UI = 14.6-27.4) and the PAF (PAF = 20.9, 95% UI = 11.2 - 30.5) measures revealed substantial absolute and relative regional inequality between the regions.</p><p><strong>Conclusion: </strong>There was a steady increase in contraceptive use from 20.3% in 1993 to 26.7% in 2014. Nevertheless, the percentage change is minimal. The trends of inequality indicate that inequalities in contraceptive use was evident across the dimension of age, place of residence, wealth index, education, and region. Yet, there was a substantial reduction in inequalities related to contraceptive use in 2014. Therefore, targeting adolescents, women in rural areas, low wealth quintile, and those with no formal education is key to substantially improving contraceptive use across the country.</p>","PeriodicalId":10637,"journal":{"name":"Contraception and Reproductive Medicine","volume":"8 1","pages":"20"},"PeriodicalIF":0.0000,"publicationDate":"2023-02-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9903545/pdf/","citationCount":"0","resultStr":"{\"title\":\"Age, geographical and socio-economic related inequalities in contraceptive prevalence: evidence from the 1993-2014 Ghana Demographic and Health Surveys.\",\"authors\":\"Felix Mensah, Joshua Okyere, Simon Agongo Azure, Eugene Budu, Edward Kwabena Ameyaw, Abdul-Aziz Seidu, Bright Opoku Ahinkorah\",\"doi\":\"10.1186/s40834-022-00194-9\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Contraceptives afford individuals the opportunity to meet their reproductive needs and reduce maternal mortality. We aimed at assessing the trend and inequalities of contraceptive use in Ghana based on the 1993-2014 Ghana Demographic and Health Surveys.</p><p><strong>Methods: </strong>We used the World Health Organization's Health Equity Assessment Toolkit (HEAT) software in analysing the data. We adopted two approaches for the analysis. First, we disaggregated inequalities in contraceptive use using four equity stratifiers: wealth index, education, residence, and region. Second, summary measures (D), (PAR), (R), and (PAF) were also employed. A 95% uncertainty interval (UI) was constructed for point estimates to measure statistical significance.</p><p><strong>Results: </strong>Contraceptive prevalence increased from 20.3% in 1993 to 26.7% in 2014. The contraceptive prevalence among women aged 20-49 increased from 20.6% [95% UI = 19.1, 22.3] in 1993 to 26.8% [95% UI = 24.9, 28.9] in 2014 and this exceeded the increase that was recorded among those aged 15-19 (from 13% [95 UI = 8.7, 19] to 18% [95% UI = 11.5, 28.6]), in the same period. It was evident that substantial inequality existed with respect to contraceptive use, from 1993 to 2014, with widest inequality occurring in 2003 (PAF = 2.7, 95% UI = -16.6-21.9; D = 17.4, 95% UI = 12.7-22.1). In terms of wealth index, the least inequality was observed in 2014 (PAR = 1.3, 95% UI = -1-3.6; D = 5.9, 95% UI = -0.1-12). Regarding education, the widest inequality occurred in 1993 (PAF = 138.6, UI = 132.1-145.1; D = 40.1, 95% UI = 34.4-45.9). With place of residence, the widest gap in inequality occurred in 1993 (PAF = 51.2, 95% UI = 46.2-56.3; D = 15.3, 95% UI = 11.8-18.7). There was inequality in contraceptive use with respect to sub-national regions. In 2014, the Difference (D = 21, 95% UI = 14.6-27.4) and the PAF (PAF = 20.9, 95% UI = 11.2 - 30.5) measures revealed substantial absolute and relative regional inequality between the regions.</p><p><strong>Conclusion: </strong>There was a steady increase in contraceptive use from 20.3% in 1993 to 26.7% in 2014. Nevertheless, the percentage change is minimal. The trends of inequality indicate that inequalities in contraceptive use was evident across the dimension of age, place of residence, wealth index, education, and region. Yet, there was a substantial reduction in inequalities related to contraceptive use in 2014. Therefore, targeting adolescents, women in rural areas, low wealth quintile, and those with no formal education is key to substantially improving contraceptive use across the country.</p>\",\"PeriodicalId\":10637,\"journal\":{\"name\":\"Contraception and Reproductive Medicine\",\"volume\":\"8 1\",\"pages\":\"20\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-02-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9903545/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Contraception and Reproductive Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s40834-022-00194-9\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Contraception and Reproductive Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40834-022-00194-9","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Age, geographical and socio-economic related inequalities in contraceptive prevalence: evidence from the 1993-2014 Ghana Demographic and Health Surveys.
Background: Contraceptives afford individuals the opportunity to meet their reproductive needs and reduce maternal mortality. We aimed at assessing the trend and inequalities of contraceptive use in Ghana based on the 1993-2014 Ghana Demographic and Health Surveys.
Methods: We used the World Health Organization's Health Equity Assessment Toolkit (HEAT) software in analysing the data. We adopted two approaches for the analysis. First, we disaggregated inequalities in contraceptive use using four equity stratifiers: wealth index, education, residence, and region. Second, summary measures (D), (PAR), (R), and (PAF) were also employed. A 95% uncertainty interval (UI) was constructed for point estimates to measure statistical significance.
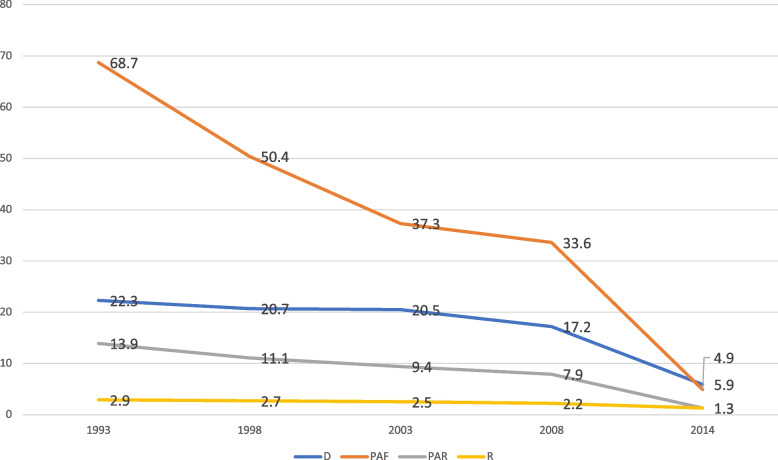
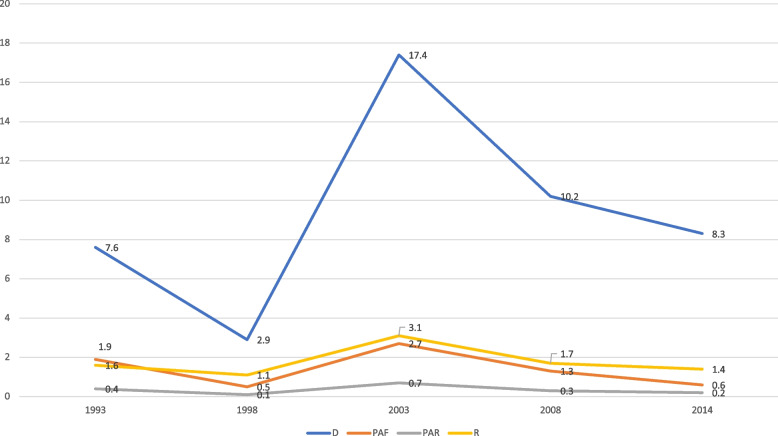
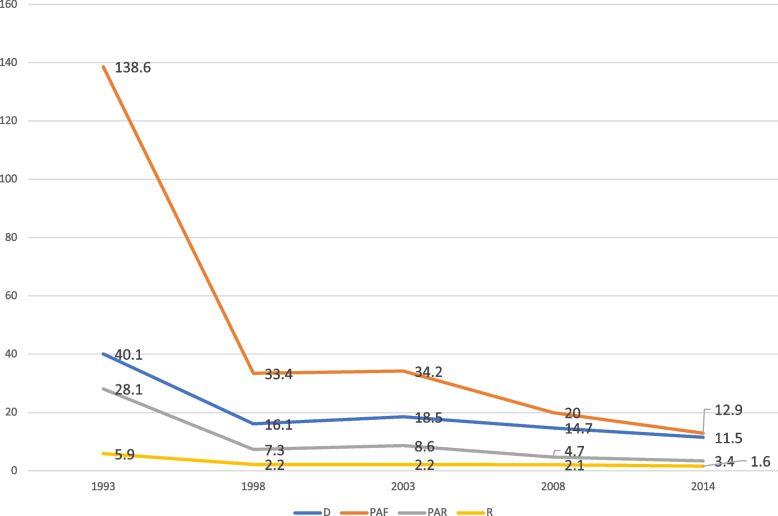
Results: Contraceptive prevalence increased from 20.3% in 1993 to 26.7% in 2014. The contraceptive prevalence among women aged 20-49 increased from 20.6% [95% UI = 19.1, 22.3] in 1993 to 26.8% [95% UI = 24.9, 28.9] in 2014 and this exceeded the increase that was recorded among those aged 15-19 (from 13% [95 UI = 8.7, 19] to 18% [95% UI = 11.5, 28.6]), in the same period. It was evident that substantial inequality existed with respect to contraceptive use, from 1993 to 2014, with widest inequality occurring in 2003 (PAF = 2.7, 95% UI = -16.6-21.9; D = 17.4, 95% UI = 12.7-22.1). In terms of wealth index, the least inequality was observed in 2014 (PAR = 1.3, 95% UI = -1-3.6; D = 5.9, 95% UI = -0.1-12). Regarding education, the widest inequality occurred in 1993 (PAF = 138.6, UI = 132.1-145.1; D = 40.1, 95% UI = 34.4-45.9). With place of residence, the widest gap in inequality occurred in 1993 (PAF = 51.2, 95% UI = 46.2-56.3; D = 15.3, 95% UI = 11.8-18.7). There was inequality in contraceptive use with respect to sub-national regions. In 2014, the Difference (D = 21, 95% UI = 14.6-27.4) and the PAF (PAF = 20.9, 95% UI = 11.2 - 30.5) measures revealed substantial absolute and relative regional inequality between the regions.
Conclusion: There was a steady increase in contraceptive use from 20.3% in 1993 to 26.7% in 2014. Nevertheless, the percentage change is minimal. The trends of inequality indicate that inequalities in contraceptive use was evident across the dimension of age, place of residence, wealth index, education, and region. Yet, there was a substantial reduction in inequalities related to contraceptive use in 2014. Therefore, targeting adolescents, women in rural areas, low wealth quintile, and those with no formal education is key to substantially improving contraceptive use across the country.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


