Shanshan Xiong, Jinshen He, Baili Chen, Yao He, Zhirong Zeng, Minhu Chen, Zhihui Chen, Yun Qiu, Ren Mao
{"title":"将回肠和吻合口病变分别纳入列线图,以预测回肠结肠切除术后克罗恩病的长期预后。","authors":"Shanshan Xiong, Jinshen He, Baili Chen, Yao He, Zhirong Zeng, Minhu Chen, Zhihui Chen, Yun Qiu, Ren Mao","doi":"10.1177/17562848231198933","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The Rutgeerts score (RS) is widely used to predict postoperative recurrence after ileocolonic resection for Crohn's disease (CD) based on the severity of lesions at the neoterminal ileum and anastomosis (RS i0-i4). However, the value of anastomotic ulcers remains controversial.</p><p><strong>Objectives: </strong>Our aim was to establish a nomogram model incorporating ileal and anastomotic lesions separately to predict the long-term outcomes of CD after ileal or ileocolonic resection.</p><p><strong>Design: </strong>A total of 136 patients with CD were included in this retrospective cohort study.</p><p><strong>Methods: </strong>Consecutive CD patients who underwent ileal or ileocolonic resections with postoperative ileocolonoscopy evaluation within 1 year after the surgery were included. The primary endpoint was postoperative clinical relapse (CR). An endoscopic classification separating ileal and anastomotic lesions was applied (Ix for neoterminal ileum lesions; Ax for anastomotic lesions). A nomogram was constructed to predict CR. The performance of the model was evaluated by the receiver-operating characteristic (ROC) curve and decision curve analysis (DCA).</p><p><strong>Results: </strong>CR was observed in 47.1% (<i>n</i> = 64) of patients within a median follow-up of 26.9 (interquartile range, 11.4-55.2) months. The risk of CR was significantly higher in patients with an RS ⩾ i2 assessed by the first postoperative endoscopy compared with patients with an RS ⩽ i1 (<i>p</i> < 0.001). Moreover, the cumulative rate of CR was significantly higher in patients with ileal lesions (I1-4) compared with patients without (I0) (<i>p</i> < 0.001). Besides, patients with anastomotic lesions (A1-3) had significantly higher rates of CR than patients without (A0) (<i>p</i> = 0.002). A nomogram, incorporating scores of postoperative ileal or anastomotic lesions, sex, L2-subtype and perianal disease, was established. The DCA analysis indicated that the nomogram had a higher benefit for CR, especially at the timeframe of 24-60 months after index endoscopy, compared to the traditional RS score.</p><p><strong>Conclusion: </strong>A nomogram incorporating postoperative ileal and anastomotic lesions separately was developed to predict CR in CD patients, which may serve as a practical tool to identify high-risk patients who need timely postoperative intervention.</p>","PeriodicalId":23022,"journal":{"name":"Therapeutic Advances in Gastroenterology","volume":"16 ","pages":"17562848231198933"},"PeriodicalIF":3.4000,"publicationDate":"2023-09-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/74/6b/10.1177_17562848231198933.PMC10503285.pdf","citationCount":"0","resultStr":"{\"title\":\"A nomogram incorporating ileal and anastomotic lesions separately to predict the long-term outcome of Crohn's disease after ileocolonic resection.\",\"authors\":\"Shanshan Xiong, Jinshen He, Baili Chen, Yao He, Zhirong Zeng, Minhu Chen, Zhihui Chen, Yun Qiu, Ren Mao\",\"doi\":\"10.1177/17562848231198933\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The Rutgeerts score (RS) is widely used to predict postoperative recurrence after ileocolonic resection for Crohn's disease (CD) based on the severity of lesions at the neoterminal ileum and anastomosis (RS i0-i4). However, the value of anastomotic ulcers remains controversial.</p><p><strong>Objectives: </strong>Our aim was to establish a nomogram model incorporating ileal and anastomotic lesions separately to predict the long-term outcomes of CD after ileal or ileocolonic resection.</p><p><strong>Design: </strong>A total of 136 patients with CD were included in this retrospective cohort study.</p><p><strong>Methods: </strong>Consecutive CD patients who underwent ileal or ileocolonic resections with postoperative ileocolonoscopy evaluation within 1 year after the surgery were included. The primary endpoint was postoperative clinical relapse (CR). An endoscopic classification separating ileal and anastomotic lesions was applied (Ix for neoterminal ileum lesions; Ax for anastomotic lesions). A nomogram was constructed to predict CR. The performance of the model was evaluated by the receiver-operating characteristic (ROC) curve and decision curve analysis (DCA).</p><p><strong>Results: </strong>CR was observed in 47.1% (<i>n</i> = 64) of patients within a median follow-up of 26.9 (interquartile range, 11.4-55.2) months. The risk of CR was significantly higher in patients with an RS ⩾ i2 assessed by the first postoperative endoscopy compared with patients with an RS ⩽ i1 (<i>p</i> < 0.001). Moreover, the cumulative rate of CR was significantly higher in patients with ileal lesions (I1-4) compared with patients without (I0) (<i>p</i> < 0.001). Besides, patients with anastomotic lesions (A1-3) had significantly higher rates of CR than patients without (A0) (<i>p</i> = 0.002). A nomogram, incorporating scores of postoperative ileal or anastomotic lesions, sex, L2-subtype and perianal disease, was established. The DCA analysis indicated that the nomogram had a higher benefit for CR, especially at the timeframe of 24-60 months after index endoscopy, compared to the traditional RS score.</p><p><strong>Conclusion: </strong>A nomogram incorporating postoperative ileal and anastomotic lesions separately was developed to predict CR in CD patients, which may serve as a practical tool to identify high-risk patients who need timely postoperative intervention.</p>\",\"PeriodicalId\":23022,\"journal\":{\"name\":\"Therapeutic Advances in Gastroenterology\",\"volume\":\"16 \",\"pages\":\"17562848231198933\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2023-09-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/74/6b/10.1177_17562848231198933.PMC10503285.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Therapeutic Advances in Gastroenterology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/17562848231198933\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Gastroenterology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/17562848231198933","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:Rutgeerts评分(RS)被广泛用于根据新末端回肠和吻合口病变的严重程度预测克罗恩病(CD)回肠结肠切除术后复发(RS i0-i4)。然而,吻合口溃疡的价值仍然存在争议。目的:我们的目的是建立一个分别包含回肠和吻合口病变的列线图模型,以预测回肠或回肠结肠切除术后CD的长期结果。设计:本回顾性队列研究共纳入136例CD患者。方法:连续接受回肠或回肠结肠切除术的CD患者在1年内进行术后回肠结肠镜检查评估 包括手术后一年。主要终点是术后临床复发(CR)。应用内镜分类法将回肠和吻合口病变分开(Ix表示新末端回肠病变;Ax表示吻合口病变)。建立了预测CR的列线图,通过受试者操作特征曲线(ROC)和决策曲线分析(DCA)对模型的性能进行了评价 = 64)的患者中位随访26.9个月(四分位间距11.4-5.2)。RS患者发生CR的风险明显更高 ⩾ i2通过术后第一次内窥镜检查与RS患者的比较 ⩽ i1(p p p = 0.002)。建立列线图,包括术后回肠或吻合口病变、性别、L2亚型和肛周疾病的评分。DCA分析表明,列线图对CR有更高的益处,尤其是在24-60的时间段 与传统的RS评分相比。结论:建立了一个分别结合术后回肠和吻合口病变的列线图来预测CD患者的CR,该列线图可作为识别需要及时术后干预的高危患者的实用工具。
A nomogram incorporating ileal and anastomotic lesions separately to predict the long-term outcome of Crohn's disease after ileocolonic resection.
Background: The Rutgeerts score (RS) is widely used to predict postoperative recurrence after ileocolonic resection for Crohn's disease (CD) based on the severity of lesions at the neoterminal ileum and anastomosis (RS i0-i4). However, the value of anastomotic ulcers remains controversial.
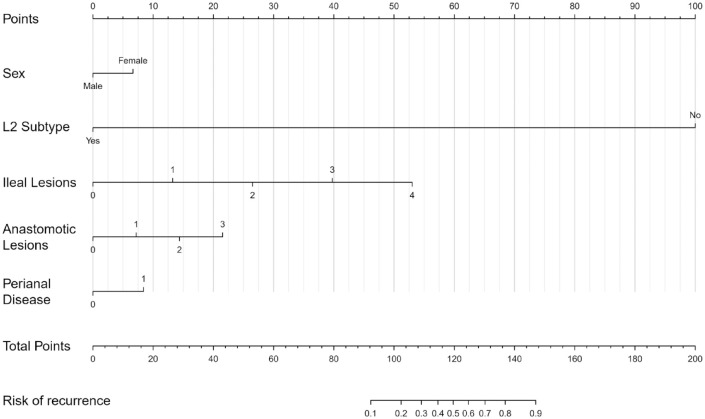
Objectives: Our aim was to establish a nomogram model incorporating ileal and anastomotic lesions separately to predict the long-term outcomes of CD after ileal or ileocolonic resection.
Design: A total of 136 patients with CD were included in this retrospective cohort study.
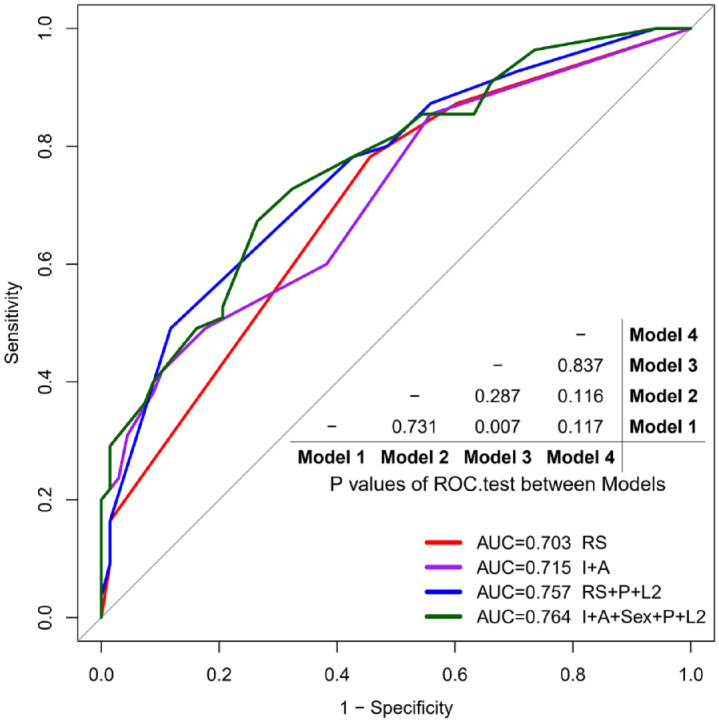
Methods: Consecutive CD patients who underwent ileal or ileocolonic resections with postoperative ileocolonoscopy evaluation within 1 year after the surgery were included. The primary endpoint was postoperative clinical relapse (CR). An endoscopic classification separating ileal and anastomotic lesions was applied (Ix for neoterminal ileum lesions; Ax for anastomotic lesions). A nomogram was constructed to predict CR. The performance of the model was evaluated by the receiver-operating characteristic (ROC) curve and decision curve analysis (DCA).
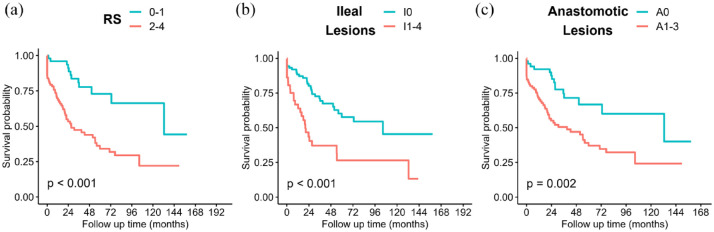
Results: CR was observed in 47.1% (n = 64) of patients within a median follow-up of 26.9 (interquartile range, 11.4-55.2) months. The risk of CR was significantly higher in patients with an RS ⩾ i2 assessed by the first postoperative endoscopy compared with patients with an RS ⩽ i1 (p < 0.001). Moreover, the cumulative rate of CR was significantly higher in patients with ileal lesions (I1-4) compared with patients without (I0) (p < 0.001). Besides, patients with anastomotic lesions (A1-3) had significantly higher rates of CR than patients without (A0) (p = 0.002). A nomogram, incorporating scores of postoperative ileal or anastomotic lesions, sex, L2-subtype and perianal disease, was established. The DCA analysis indicated that the nomogram had a higher benefit for CR, especially at the timeframe of 24-60 months after index endoscopy, compared to the traditional RS score.
Conclusion: A nomogram incorporating postoperative ileal and anastomotic lesions separately was developed to predict CR in CD patients, which may serve as a practical tool to identify high-risk patients who need timely postoperative intervention.
期刊介绍:
Therapeutic Advances in Gastroenterology is an open access journal which delivers the highest quality peer-reviewed original research articles, reviews, and scholarly comment on pioneering efforts and innovative studies in the medical treatment of gastrointestinal and hepatic disorders. The journal has a strong clinical and pharmacological focus and is aimed at an international audience of clinicians and researchers in gastroenterology and related disciplines, providing an online forum for rapid dissemination of recent research and perspectives in this area.
The editors welcome original research articles across all areas of gastroenterology and hepatology.
The journal publishes original research articles and review articles primarily. Original research manuscripts may include laboratory, animal or human/clinical studies – all phases. Letters to the Editor and Case Reports will also be considered.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


