Louis Boutin, Louis Morisson, Florence Riché, Romain Barthélémy, Alexandre Mebazaa, Philippe Soyer, Benoit Gallix, Anthony Dohan, Benjamin G Chousterman
{"title":"法国重症监护室消化源性败血症期间腹部器官放射组学分析。","authors":"Louis Boutin, Louis Morisson, Florence Riché, Romain Barthélémy, Alexandre Mebazaa, Philippe Soyer, Benoit Gallix, Anthony Dohan, Benjamin G Chousterman","doi":"10.4266/acc.2023.00136","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Sepsis is a severe and common cause of admission to the intensive care unit (ICU). Radiomic analysis (RA) may predict organ failure and patient outcomes. The objective of this study was to assess a model of RA and to evaluate its performance in predicting in-ICU mortality and acute kidney injury (AKI) during abdominal sepsis.</p><p><strong>Methods: </strong>This single-center, retrospective study included patients admitted to the ICU for abdominal sepsis. To predict in-ICU mortality or AKI, elastic net regularized logistic regression and the random forest algorithm were used in a five-fold cross-validation set repeated 10 times.</p><p><strong>Results: </strong>Fifty-five patients were included. In-ICU mortality was 25.5%, and 76.4% of patients developed AKI. To predict in-ICU mortality, elastic net and random forest models, respectively, achieved areas under the curve (AUCs) of 0.48 (95% confidence interval [CI], 0.43-0.54) and 0.51 (95% CI, 0.46-0.57) and were not improved combined with Simplified Acute Physiology Score (SAPS) II. To predict AKI with RA, the AUC was 0.71 (95% CI, 0.66-0.77) for elastic net and 0.69 (95% CI, 0.64-0.74) for random forest, and these were improved combined with SAPS II, respectively; AUC of 0.94 (95% CI, 0.91-0.96) and 0.75 (95% CI, 0.70-0.80) for elastic net and random forest, respectively.</p><p><strong>Conclusions: </strong>This study suggests that RA has poor predictive performance for in-ICU mortality but good predictive performance for AKI in patients with abdominal sepsis. A secondary validation cohort is needed to confirm these results and the assessed model.</p>","PeriodicalId":44118,"journal":{"name":"Acute and Critical Care","volume":"38 3","pages":"343-352"},"PeriodicalIF":1.7000,"publicationDate":"2023-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1f/cf/acc-2023-00136.PMC10497895.pdf","citationCount":"0","resultStr":"{\"title\":\"Radiomic analysis of abdominal organs during sepsis of digestive origin in a French intensive care unit.\",\"authors\":\"Louis Boutin, Louis Morisson, Florence Riché, Romain Barthélémy, Alexandre Mebazaa, Philippe Soyer, Benoit Gallix, Anthony Dohan, Benjamin G Chousterman\",\"doi\":\"10.4266/acc.2023.00136\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Sepsis is a severe and common cause of admission to the intensive care unit (ICU). Radiomic analysis (RA) may predict organ failure and patient outcomes. The objective of this study was to assess a model of RA and to evaluate its performance in predicting in-ICU mortality and acute kidney injury (AKI) during abdominal sepsis.</p><p><strong>Methods: </strong>This single-center, retrospective study included patients admitted to the ICU for abdominal sepsis. To predict in-ICU mortality or AKI, elastic net regularized logistic regression and the random forest algorithm were used in a five-fold cross-validation set repeated 10 times.</p><p><strong>Results: </strong>Fifty-five patients were included. In-ICU mortality was 25.5%, and 76.4% of patients developed AKI. To predict in-ICU mortality, elastic net and random forest models, respectively, achieved areas under the curve (AUCs) of 0.48 (95% confidence interval [CI], 0.43-0.54) and 0.51 (95% CI, 0.46-0.57) and were not improved combined with Simplified Acute Physiology Score (SAPS) II. To predict AKI with RA, the AUC was 0.71 (95% CI, 0.66-0.77) for elastic net and 0.69 (95% CI, 0.64-0.74) for random forest, and these were improved combined with SAPS II, respectively; AUC of 0.94 (95% CI, 0.91-0.96) and 0.75 (95% CI, 0.70-0.80) for elastic net and random forest, respectively.</p><p><strong>Conclusions: </strong>This study suggests that RA has poor predictive performance for in-ICU mortality but good predictive performance for AKI in patients with abdominal sepsis. A secondary validation cohort is needed to confirm these results and the assessed model.</p>\",\"PeriodicalId\":44118,\"journal\":{\"name\":\"Acute and Critical Care\",\"volume\":\"38 3\",\"pages\":\"343-352\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2023-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1f/cf/acc-2023-00136.PMC10497895.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Acute and Critical Care\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4266/acc.2023.00136\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acute and Critical Care","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4266/acc.2023.00136","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
Radiomic analysis of abdominal organs during sepsis of digestive origin in a French intensive care unit.
Background: Sepsis is a severe and common cause of admission to the intensive care unit (ICU). Radiomic analysis (RA) may predict organ failure and patient outcomes. The objective of this study was to assess a model of RA and to evaluate its performance in predicting in-ICU mortality and acute kidney injury (AKI) during abdominal sepsis.
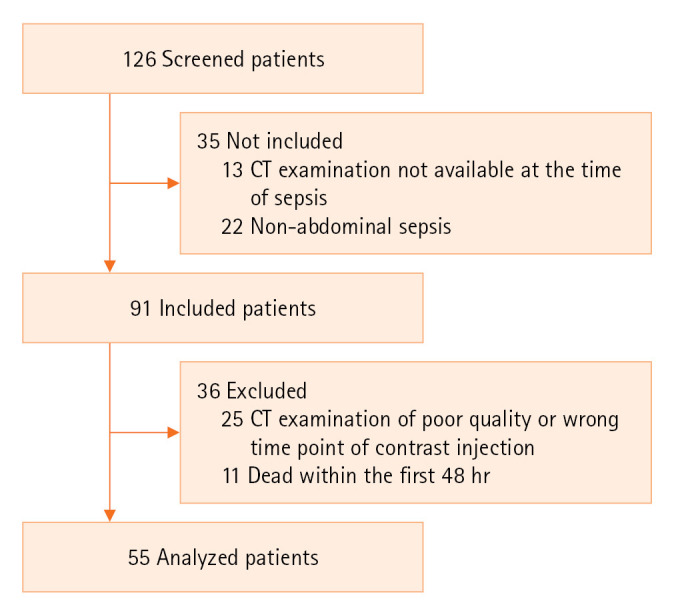
Methods: This single-center, retrospective study included patients admitted to the ICU for abdominal sepsis. To predict in-ICU mortality or AKI, elastic net regularized logistic regression and the random forest algorithm were used in a five-fold cross-validation set repeated 10 times.
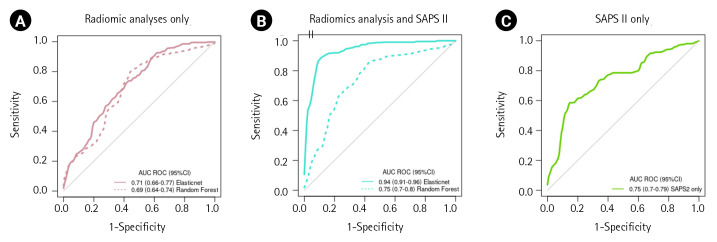
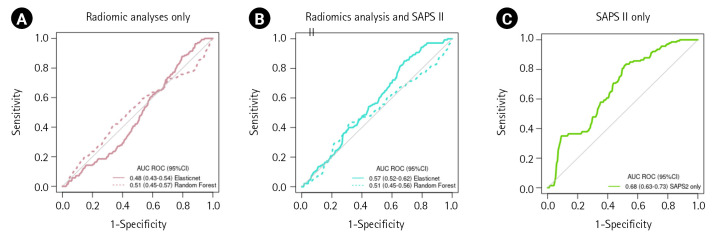
Results: Fifty-five patients were included. In-ICU mortality was 25.5%, and 76.4% of patients developed AKI. To predict in-ICU mortality, elastic net and random forest models, respectively, achieved areas under the curve (AUCs) of 0.48 (95% confidence interval [CI], 0.43-0.54) and 0.51 (95% CI, 0.46-0.57) and were not improved combined with Simplified Acute Physiology Score (SAPS) II. To predict AKI with RA, the AUC was 0.71 (95% CI, 0.66-0.77) for elastic net and 0.69 (95% CI, 0.64-0.74) for random forest, and these were improved combined with SAPS II, respectively; AUC of 0.94 (95% CI, 0.91-0.96) and 0.75 (95% CI, 0.70-0.80) for elastic net and random forest, respectively.
Conclusions: This study suggests that RA has poor predictive performance for in-ICU mortality but good predictive performance for AKI in patients with abdominal sepsis. A secondary validation cohort is needed to confirm these results and the assessed model.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


