{"title":"免疫检查点抑制剂治疗相关肠炎模拟乳糜泻。","authors":"Binny Khandakar, Amitabh Srivastava","doi":"10.22037/ghfbb.v16i2.2855","DOIUrl":null,"url":null,"abstract":"<p><p>A 68-year-old man with a previous history of lung cancer presented with deteriorating appetite and weight loss. Imaging revealed significant retroperitoneal lymphadenopathy, as well as liver and bone lesions consistent with widespread metastatic carcinoma. Biopsy results from the liver lesions confirmed the diagnosis of metastatic non-small cell lung carcinoma. A PDL-1 immunostain, performed on the initial lung resection specimen, showed a combined positive score (CPS) of 15 and pembrolizumab treatment was initiated. The patient presented with diarrhea three weeks after starting therapy and duodenal biopsies obtained at this time displayed intact villous architecture with an increase in intraepithelial lymphocytes (IELs). The colon biopsies exhibited lymphocytic colitis, characterized by significant thinning of the surface epithelium, a higher mixed inflammatory infiltrate within the lamina propria, and diffuse increase of IELs (greater than 30 per 100 epithelial cells). These findings collectively raised the differential diagnosis of celiac disease with lymphocytic colitis or immunotherapy-associated enterocolitis. Further serological testing for celiac disease, including anti-tissue transglutaminase antibodies, yielded negative results. Consequently, a final diagnosis of immune adverse event associated with immunotherapy was established. Cases reported in literature as celiac disease occurring soon after immunotherapy are likely misdiagnosed cases of immunotherapy enteritis.</p>","PeriodicalId":12636,"journal":{"name":"Gastroenterology and Hepatology From Bed to Bench","volume":"16 2","pages":"240-244"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/7c/1f/GHFBB-16-240.PMC10404836.pdf","citationCount":"0","resultStr":"{\"title\":\"Immune checkpoint inhibitor therapy associated enteritis mimicking celiac disease.\",\"authors\":\"Binny Khandakar, Amitabh Srivastava\",\"doi\":\"10.22037/ghfbb.v16i2.2855\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>A 68-year-old man with a previous history of lung cancer presented with deteriorating appetite and weight loss. Imaging revealed significant retroperitoneal lymphadenopathy, as well as liver and bone lesions consistent with widespread metastatic carcinoma. Biopsy results from the liver lesions confirmed the diagnosis of metastatic non-small cell lung carcinoma. A PDL-1 immunostain, performed on the initial lung resection specimen, showed a combined positive score (CPS) of 15 and pembrolizumab treatment was initiated. The patient presented with diarrhea three weeks after starting therapy and duodenal biopsies obtained at this time displayed intact villous architecture with an increase in intraepithelial lymphocytes (IELs). The colon biopsies exhibited lymphocytic colitis, characterized by significant thinning of the surface epithelium, a higher mixed inflammatory infiltrate within the lamina propria, and diffuse increase of IELs (greater than 30 per 100 epithelial cells). These findings collectively raised the differential diagnosis of celiac disease with lymphocytic colitis or immunotherapy-associated enterocolitis. Further serological testing for celiac disease, including anti-tissue transglutaminase antibodies, yielded negative results. Consequently, a final diagnosis of immune adverse event associated with immunotherapy was established. Cases reported in literature as celiac disease occurring soon after immunotherapy are likely misdiagnosed cases of immunotherapy enteritis.</p>\",\"PeriodicalId\":12636,\"journal\":{\"name\":\"Gastroenterology and Hepatology From Bed to Bench\",\"volume\":\"16 2\",\"pages\":\"240-244\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/7c/1f/GHFBB-16-240.PMC10404836.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Gastroenterology and Hepatology From Bed to Bench\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.22037/ghfbb.v16i2.2855\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Gastroenterology and Hepatology From Bed to Bench","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22037/ghfbb.v16i2.2855","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
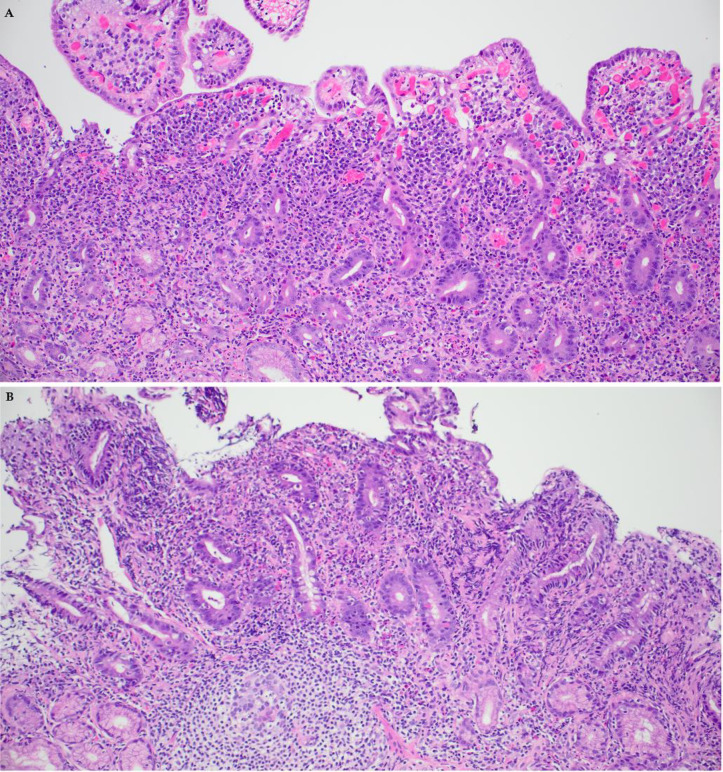
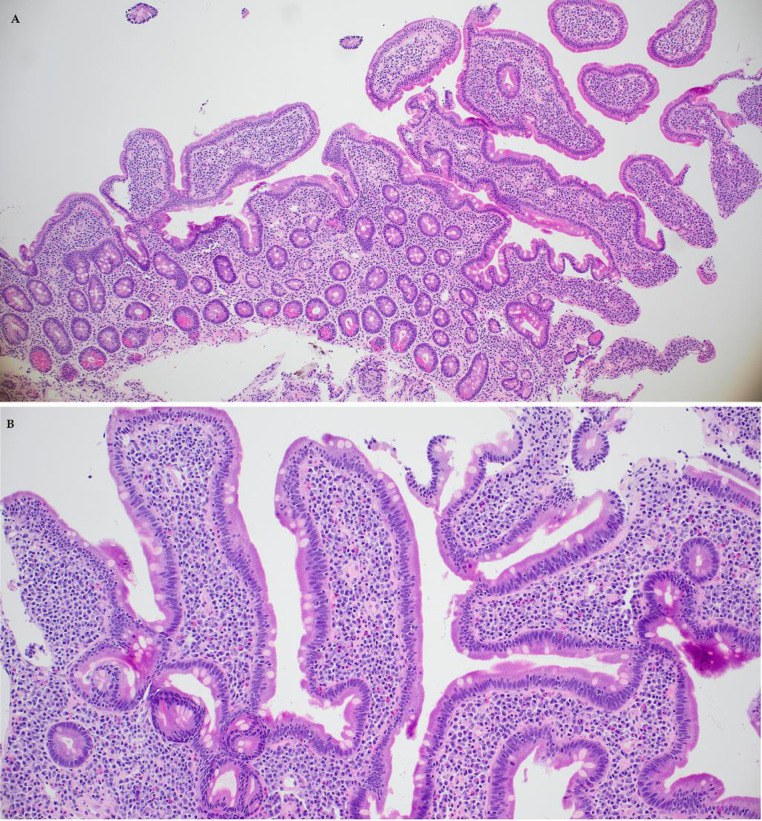
A 68-year-old man with a previous history of lung cancer presented with deteriorating appetite and weight loss. Imaging revealed significant retroperitoneal lymphadenopathy, as well as liver and bone lesions consistent with widespread metastatic carcinoma. Biopsy results from the liver lesions confirmed the diagnosis of metastatic non-small cell lung carcinoma. A PDL-1 immunostain, performed on the initial lung resection specimen, showed a combined positive score (CPS) of 15 and pembrolizumab treatment was initiated. The patient presented with diarrhea three weeks after starting therapy and duodenal biopsies obtained at this time displayed intact villous architecture with an increase in intraepithelial lymphocytes (IELs). The colon biopsies exhibited lymphocytic colitis, characterized by significant thinning of the surface epithelium, a higher mixed inflammatory infiltrate within the lamina propria, and diffuse increase of IELs (greater than 30 per 100 epithelial cells). These findings collectively raised the differential diagnosis of celiac disease with lymphocytic colitis or immunotherapy-associated enterocolitis. Further serological testing for celiac disease, including anti-tissue transglutaminase antibodies, yielded negative results. Consequently, a final diagnosis of immune adverse event associated with immunotherapy was established. Cases reported in literature as celiac disease occurring soon after immunotherapy are likely misdiagnosed cases of immunotherapy enteritis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


