Molly Dreher, Jungwon Min, Constantine Mavroudis, Douglas Ryba, Svetlana Ostapenko, Richard Melchior, Tami Rosenthal, Muhammad Nuri, Joshua Blinder
{"title":"小儿体外循环期间指数化供氧是术后急性肾损伤的一个可改变的危险因素。","authors":"Molly Dreher, Jungwon Min, Constantine Mavroudis, Douglas Ryba, Svetlana Ostapenko, Richard Melchior, Tami Rosenthal, Muhammad Nuri, Joshua Blinder","doi":"10.1051/ject/2023029","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Acute kidney injury after pediatric cardiac surgery is a common complication with few established modifiable risk factors. We sought to characterize whether indexed oxygen delivery during cardiopulmonary bypass was associated with postoperative acute kidney injury in a large pediatric cohort.</p><p><strong>Methods: </strong>This was a retrospective analysis of patients under 1 year old undergoing cardiac surgery with cardiopulmonary bypass between January 1, 2013, and January 1, 2020. Receiver operating characteristic curves across values ranging from 260 to 400 mL/min/m<sup>2</sup> were used to identify the indexed oxygen delivery most significantly associated with acute kidney injury risk.</p><p><strong>Results: </strong>We included 980 patients with acute kidney injury occurring in 212 (21.2%). After adjusting for covariates associated with acute kidney injury, an indexed oxygen delivery threshold of 340 mL/min/m<sup>2</sup> predicted acute kidney injury in STAT 4 and 5 neonates (area under the curve = 0.66, 95% CI = 0.60 - 0.72, sensitivity = 56.1%, specificity = 69.4%). An indexed oxygen delivery threshold of 400 mL/min/m<sup>2</sup> predicted acute kidney injury in STAT 1-3 infants (area under the curve = 0.65, 95% CI = 0.58 - 0.72, sensitivity = 52.6%, specificity = 74.6%).</p><p><strong>Conclusion: </strong>Indexed oxygen delivery during cardiopulmonary bypass is a modifiable variable independently associated with postoperative acute kidney injury in specific pediatric populations. Strategies aimed at maintaining oxygen delivery greater than 340 mL/min/m<sup>2</sup> in complex neonates and greater than 400 mL/min/m<sup>2</sup> in infants may reduce the occurrence of postoperative acute kidney injury in the pediatric population.</p>","PeriodicalId":39644,"journal":{"name":"Journal of Extra-Corporeal Technology","volume":"55 3","pages":"112-120"},"PeriodicalIF":0.0000,"publicationDate":"2023-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10487348/pdf/","citationCount":"0","resultStr":"{\"title\":\"Indexed oxygen delivery during pediatric cardiopulmonary bypass is a modifiable risk factor for postoperative acute kidney injury.\",\"authors\":\"Molly Dreher, Jungwon Min, Constantine Mavroudis, Douglas Ryba, Svetlana Ostapenko, Richard Melchior, Tami Rosenthal, Muhammad Nuri, Joshua Blinder\",\"doi\":\"10.1051/ject/2023029\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Acute kidney injury after pediatric cardiac surgery is a common complication with few established modifiable risk factors. We sought to characterize whether indexed oxygen delivery during cardiopulmonary bypass was associated with postoperative acute kidney injury in a large pediatric cohort.</p><p><strong>Methods: </strong>This was a retrospective analysis of patients under 1 year old undergoing cardiac surgery with cardiopulmonary bypass between January 1, 2013, and January 1, 2020. Receiver operating characteristic curves across values ranging from 260 to 400 mL/min/m<sup>2</sup> were used to identify the indexed oxygen delivery most significantly associated with acute kidney injury risk.</p><p><strong>Results: </strong>We included 980 patients with acute kidney injury occurring in 212 (21.2%). After adjusting for covariates associated with acute kidney injury, an indexed oxygen delivery threshold of 340 mL/min/m<sup>2</sup> predicted acute kidney injury in STAT 4 and 5 neonates (area under the curve = 0.66, 95% CI = 0.60 - 0.72, sensitivity = 56.1%, specificity = 69.4%). An indexed oxygen delivery threshold of 400 mL/min/m<sup>2</sup> predicted acute kidney injury in STAT 1-3 infants (area under the curve = 0.65, 95% CI = 0.58 - 0.72, sensitivity = 52.6%, specificity = 74.6%).</p><p><strong>Conclusion: </strong>Indexed oxygen delivery during cardiopulmonary bypass is a modifiable variable independently associated with postoperative acute kidney injury in specific pediatric populations. Strategies aimed at maintaining oxygen delivery greater than 340 mL/min/m<sup>2</sup> in complex neonates and greater than 400 mL/min/m<sup>2</sup> in infants may reduce the occurrence of postoperative acute kidney injury in the pediatric population.</p>\",\"PeriodicalId\":39644,\"journal\":{\"name\":\"Journal of Extra-Corporeal Technology\",\"volume\":\"55 3\",\"pages\":\"112-120\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10487348/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Extra-Corporeal Technology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1051/ject/2023029\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"Health Professions\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Extra-Corporeal Technology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1051/ject/2023029","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Health Professions","Score":null,"Total":0}
Indexed oxygen delivery during pediatric cardiopulmonary bypass is a modifiable risk factor for postoperative acute kidney injury.
Background: Acute kidney injury after pediatric cardiac surgery is a common complication with few established modifiable risk factors. We sought to characterize whether indexed oxygen delivery during cardiopulmonary bypass was associated with postoperative acute kidney injury in a large pediatric cohort.
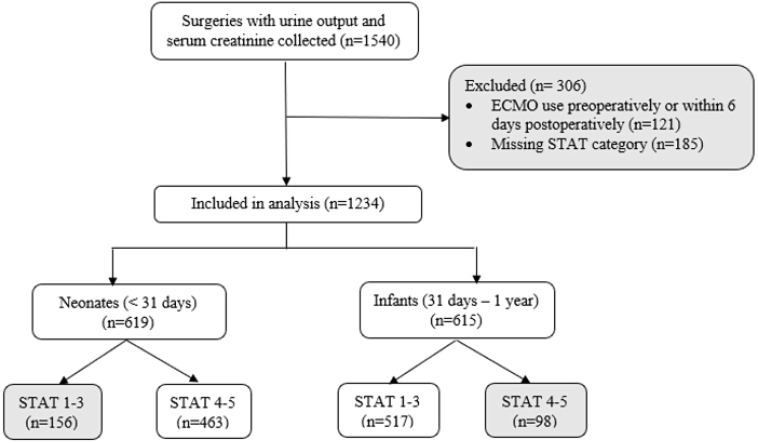
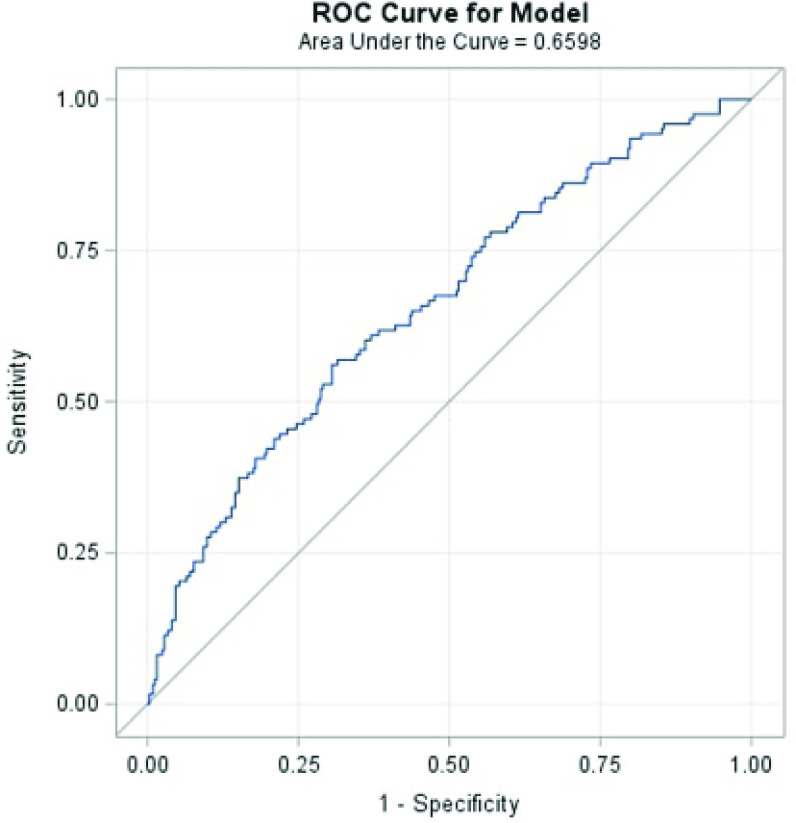
Methods: This was a retrospective analysis of patients under 1 year old undergoing cardiac surgery with cardiopulmonary bypass between January 1, 2013, and January 1, 2020. Receiver operating characteristic curves across values ranging from 260 to 400 mL/min/m2 were used to identify the indexed oxygen delivery most significantly associated with acute kidney injury risk.
Results: We included 980 patients with acute kidney injury occurring in 212 (21.2%). After adjusting for covariates associated with acute kidney injury, an indexed oxygen delivery threshold of 340 mL/min/m2 predicted acute kidney injury in STAT 4 and 5 neonates (area under the curve = 0.66, 95% CI = 0.60 - 0.72, sensitivity = 56.1%, specificity = 69.4%). An indexed oxygen delivery threshold of 400 mL/min/m2 predicted acute kidney injury in STAT 1-3 infants (area under the curve = 0.65, 95% CI = 0.58 - 0.72, sensitivity = 52.6%, specificity = 74.6%).
Conclusion: Indexed oxygen delivery during cardiopulmonary bypass is a modifiable variable independently associated with postoperative acute kidney injury in specific pediatric populations. Strategies aimed at maintaining oxygen delivery greater than 340 mL/min/m2 in complex neonates and greater than 400 mL/min/m2 in infants may reduce the occurrence of postoperative acute kidney injury in the pediatric population.
期刊介绍:
The Journal of Extracorporeal Technology is dedicated to the study and practice of Basic Science and Clinical issues related to extracorporeal circulation. Areas emphasized in the Journal include: •Cardiopulmonary Bypass •Cardiac Surgery •Cardiovascular Anesthesia •Hematology •Blood Management •Physiology •Fluid Dynamics •Laboratory Science •Coagulation and Hematology •Transfusion •Business Practices •Pediatric Perfusion •Total Quality Management • Evidence-Based Practices


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


