Ietje T Hazenberg, Stephanie J M Middelkoop, Anoek A E de Joode, Juliette D Rabbeljee, Robert A Pol, Benjamin H J Doornweerd, Jan-Stephan F Sanders, Coen A Stegeman
{"title":"输尿管外支架与肾移植内双J支架:泌尿系统并发症和尿路感染发生率的回顾性分析。","authors":"Ietje T Hazenberg, Stephanie J M Middelkoop, Anoek A E de Joode, Juliette D Rabbeljee, Robert A Pol, Benjamin H J Doornweerd, Jan-Stephan F Sanders, Coen A Stegeman","doi":"10.3389/fneph.2023.1130672","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Urologic complications (UCs) and urinary tract infections (UTIs) are common after kidney transplantation. Intraoperative stent placement at the vesicoureteric anastomosis reduces UC risk, but increases UTI risk.</p><p><strong>Methods: </strong>In 2014 our stenting protocol changed from external ureteric stent (ES) to internal double J stent (DJ). We retrospectively studied the occurrence of UCs and UTIs in relation to ES or DJ in 697 kidney recipients.</p><p><strong>Methods: </strong>An ES was used in 403 patients (57.8%), in 294 (42.2%) a DJ. ES was removed 7-12 days and DJ 3-4 weeks post-operative. Induction immunosuppression was the same in both groups. Primary outcomes at 6 months follow-up were UC (urinary leakage/ureter stenosis) and UTI; they were related to stenting procedure and clinical and transplant characteristics. The incidence of UCs was similar for ES (8.4%) and DJ (6.8%), p=0.389. ES use was a significant risk factor for UTI (OR 1.69 (1.15-2.50), p=0.008). Post-transplant hospitalization was significantly shorter in the DJ group. Despite more acute rejection episodes with ES (ES/DJ: 16.4%/6.1%, p<0.001), no clinical relevant differences in graft outcomes existed.</p><p><strong>Discussion: </strong>A DJ is, compared to ES, associated with a lower incidence of UTIs and comparable occurrence of UCs and is therefore the preferred technique for stenting the vesicoureteric anastomosis.</p>","PeriodicalId":73091,"journal":{"name":"Frontiers in nephrology","volume":"3 ","pages":"1130672"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10479681/pdf/","citationCount":"0","resultStr":"{\"title\":\"External ureteric stent versus internal double J stent in kidney transplantation: a retrospective analysis on the incidence of urological complications and urinary tract infections.\",\"authors\":\"Ietje T Hazenberg, Stephanie J M Middelkoop, Anoek A E de Joode, Juliette D Rabbeljee, Robert A Pol, Benjamin H J Doornweerd, Jan-Stephan F Sanders, Coen A Stegeman\",\"doi\":\"10.3389/fneph.2023.1130672\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Urologic complications (UCs) and urinary tract infections (UTIs) are common after kidney transplantation. Intraoperative stent placement at the vesicoureteric anastomosis reduces UC risk, but increases UTI risk.</p><p><strong>Methods: </strong>In 2014 our stenting protocol changed from external ureteric stent (ES) to internal double J stent (DJ). We retrospectively studied the occurrence of UCs and UTIs in relation to ES or DJ in 697 kidney recipients.</p><p><strong>Methods: </strong>An ES was used in 403 patients (57.8%), in 294 (42.2%) a DJ. ES was removed 7-12 days and DJ 3-4 weeks post-operative. Induction immunosuppression was the same in both groups. Primary outcomes at 6 months follow-up were UC (urinary leakage/ureter stenosis) and UTI; they were related to stenting procedure and clinical and transplant characteristics. The incidence of UCs was similar for ES (8.4%) and DJ (6.8%), p=0.389. ES use was a significant risk factor for UTI (OR 1.69 (1.15-2.50), p=0.008). Post-transplant hospitalization was significantly shorter in the DJ group. Despite more acute rejection episodes with ES (ES/DJ: 16.4%/6.1%, p<0.001), no clinical relevant differences in graft outcomes existed.</p><p><strong>Discussion: </strong>A DJ is, compared to ES, associated with a lower incidence of UTIs and comparable occurrence of UCs and is therefore the preferred technique for stenting the vesicoureteric anastomosis.</p>\",\"PeriodicalId\":73091,\"journal\":{\"name\":\"Frontiers in nephrology\",\"volume\":\"3 \",\"pages\":\"1130672\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10479681/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Frontiers in nephrology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3389/fneph.2023.1130672\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in nephrology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3389/fneph.2023.1130672","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
External ureteric stent versus internal double J stent in kidney transplantation: a retrospective analysis on the incidence of urological complications and urinary tract infections.
Introduction: Urologic complications (UCs) and urinary tract infections (UTIs) are common after kidney transplantation. Intraoperative stent placement at the vesicoureteric anastomosis reduces UC risk, but increases UTI risk.
Methods: In 2014 our stenting protocol changed from external ureteric stent (ES) to internal double J stent (DJ). We retrospectively studied the occurrence of UCs and UTIs in relation to ES or DJ in 697 kidney recipients.
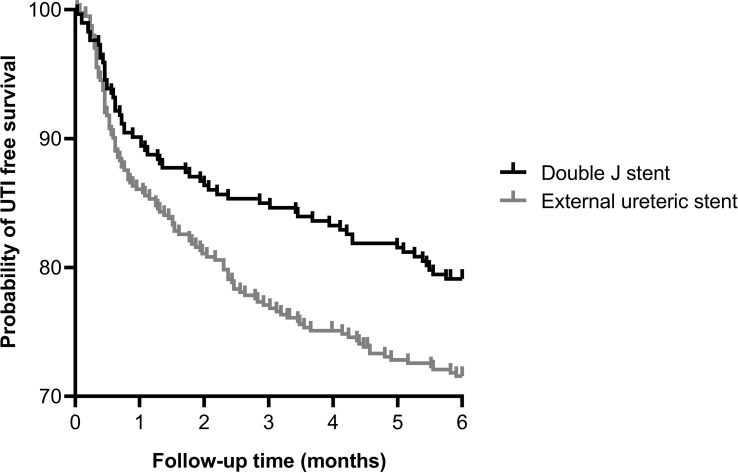
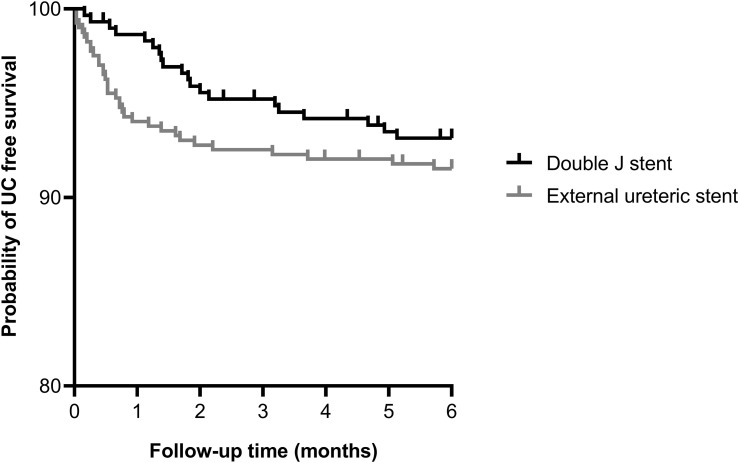
Methods: An ES was used in 403 patients (57.8%), in 294 (42.2%) a DJ. ES was removed 7-12 days and DJ 3-4 weeks post-operative. Induction immunosuppression was the same in both groups. Primary outcomes at 6 months follow-up were UC (urinary leakage/ureter stenosis) and UTI; they were related to stenting procedure and clinical and transplant characteristics. The incidence of UCs was similar for ES (8.4%) and DJ (6.8%), p=0.389. ES use was a significant risk factor for UTI (OR 1.69 (1.15-2.50), p=0.008). Post-transplant hospitalization was significantly shorter in the DJ group. Despite more acute rejection episodes with ES (ES/DJ: 16.4%/6.1%, p<0.001), no clinical relevant differences in graft outcomes existed.
Discussion: A DJ is, compared to ES, associated with a lower incidence of UTIs and comparable occurrence of UCs and is therefore the preferred technique for stenting the vesicoureteric anastomosis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


