Jacopo Ciaffi, Giancarlo Facchini, Stefano Bandiera, Carlotta Cavallari, Marco Miceli, Alessandro Gasbarrini, Francesco Ursini
{"title":"临床影像:一个快照从过去:未经治疗的强直性脊柱炎在生物时代。","authors":"Jacopo Ciaffi, Giancarlo Facchini, Stefano Bandiera, Carlotta Cavallari, Marco Miceli, Alessandro Gasbarrini, Francesco Ursini","doi":"10.1002/acr2.11492","DOIUrl":null,"url":null,"abstract":"The patient, a 48-year-old man, was referred to our rheumatology clinic for severe spinal limitation and impaired gait. The patient was born in an underprivileged country and reported a 25-year history of in fl ammatory axial and peripheral pain with progressive dis-ability. A speci fi c diagnosis had never been made, and he was treated with painkillers on demand. Radiographs showed the pres-ence of diffuse, severe musculoskeletal abnormalities. Computed tomography demonstrated total ankylosis of the spine (video and panel A, generated with three-dimensional volume rendering and bone segmentation; chest wall was removed to facilitate visualiza-tion of the spine) due to massive syndesmophytosis, ankylosis of the facet joints, and ossi fi cation of the fl avum, supraspinous, and interspinous ligaments (panel B). A possible previous vertebral compression wedge fracture was also noted at the T10-T11 level (panel B), but the patient reported no history of acute back pain or trauma. Fusion of sacroiliac joints (panel C), severe destruction with complete ankylosis and fi xed fl exion deformity of both hips at 35 degrees (panel D), and subtotal ankylosis of both shoulders (panel E) were also evident, along with widespread periarticular and entheseal ossi fi cation. The patient was diagnosed with HLA-B27 positive radiographic axial spondyloarthritis (SpA), classi fi ed as ankylosing spondylitis, and scheduled for bilateral hip and shoulder replacement.","PeriodicalId":7084,"journal":{"name":"ACR Open Rheumatology","volume":"5 1","pages":"15-16"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b2/6d/ACR2-5-15.PMC9837388.pdf","citationCount":"0","resultStr":"{\"title\":\"Clinical Images: A snapshot from the past: untreated ankylosing spondylitis in the biologic era.\",\"authors\":\"Jacopo Ciaffi, Giancarlo Facchini, Stefano Bandiera, Carlotta Cavallari, Marco Miceli, Alessandro Gasbarrini, Francesco Ursini\",\"doi\":\"10.1002/acr2.11492\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"The patient, a 48-year-old man, was referred to our rheumatology clinic for severe spinal limitation and impaired gait. The patient was born in an underprivileged country and reported a 25-year history of in fl ammatory axial and peripheral pain with progressive dis-ability. A speci fi c diagnosis had never been made, and he was treated with painkillers on demand. Radiographs showed the pres-ence of diffuse, severe musculoskeletal abnormalities. Computed tomography demonstrated total ankylosis of the spine (video and panel A, generated with three-dimensional volume rendering and bone segmentation; chest wall was removed to facilitate visualiza-tion of the spine) due to massive syndesmophytosis, ankylosis of the facet joints, and ossi fi cation of the fl avum, supraspinous, and interspinous ligaments (panel B). A possible previous vertebral compression wedge fracture was also noted at the T10-T11 level (panel B), but the patient reported no history of acute back pain or trauma. Fusion of sacroiliac joints (panel C), severe destruction with complete ankylosis and fi xed fl exion deformity of both hips at 35 degrees (panel D), and subtotal ankylosis of both shoulders (panel E) were also evident, along with widespread periarticular and entheseal ossi fi cation. The patient was diagnosed with HLA-B27 positive radiographic axial spondyloarthritis (SpA), classi fi ed as ankylosing spondylitis, and scheduled for bilateral hip and shoulder replacement.\",\"PeriodicalId\":7084,\"journal\":{\"name\":\"ACR Open Rheumatology\",\"volume\":\"5 1\",\"pages\":\"15-16\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b2/6d/ACR2-5-15.PMC9837388.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ACR Open Rheumatology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1002/acr2.11492\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ACR Open Rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1002/acr2.11492","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Clinical Images: A snapshot from the past: untreated ankylosing spondylitis in the biologic era.
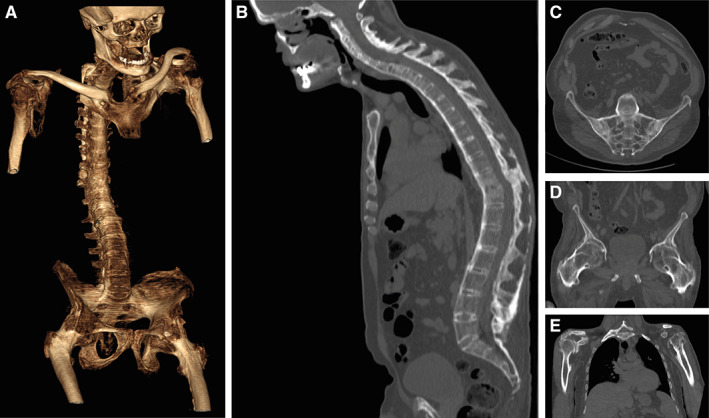
The patient, a 48-year-old man, was referred to our rheumatology clinic for severe spinal limitation and impaired gait. The patient was born in an underprivileged country and reported a 25-year history of in fl ammatory axial and peripheral pain with progressive dis-ability. A speci fi c diagnosis had never been made, and he was treated with painkillers on demand. Radiographs showed the pres-ence of diffuse, severe musculoskeletal abnormalities. Computed tomography demonstrated total ankylosis of the spine (video and panel A, generated with three-dimensional volume rendering and bone segmentation; chest wall was removed to facilitate visualiza-tion of the spine) due to massive syndesmophytosis, ankylosis of the facet joints, and ossi fi cation of the fl avum, supraspinous, and interspinous ligaments (panel B). A possible previous vertebral compression wedge fracture was also noted at the T10-T11 level (panel B), but the patient reported no history of acute back pain or trauma. Fusion of sacroiliac joints (panel C), severe destruction with complete ankylosis and fi xed fl exion deformity of both hips at 35 degrees (panel D), and subtotal ankylosis of both shoulders (panel E) were also evident, along with widespread periarticular and entheseal ossi fi cation. The patient was diagnosed with HLA-B27 positive radiographic axial spondyloarthritis (SpA), classi fi ed as ankylosing spondylitis, and scheduled for bilateral hip and shoulder replacement.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


