{"title":"在急症护理环境中,抗精神病药物单一疗法失败后的抗精神病药物处方实践比较。","authors":"Kaitlyn Morgan, Leah Rickert","doi":"10.9740/mhc.2022.12.329","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Numerous strategies exist following antipsychotic monotherapy failure including transition to another antipsychotic, dosing above FDA recommendations, or dual antipsychotic therapy. This study described antipsychotic prescribing practices on an acute psychiatry unit following antipsychotic monotherapy failure and compared outcomes to determine if any strategy resulted in superior short-term outcomes.</p><p><strong>Methods: </strong>This retrospective chart review assessed postintervention time to discharge for patients with schizophrenia or schizoaffective disorder requiring therapy change following treatment failure. Secondary outcomes included 30-day readmission rate, length of stay, and discharge chlorpromazine equivalents.</p><p><strong>Results: </strong>There were no differences in number of past antipsychotic trials between groups (4.8 vs 4.5; <i>P</i> = .73). Of all the patients, 73% (n = 30) discharged on alternative antipsychotic monotherapy while 27% (n = 11) discharged on dual antipsychotic therapy. No patients had doses increased above FDA recommendations. The alternative antipsychotic group had shorter mean postintervention time to discharge (8.8 vs 20.6 days; <i>P</i> = .003) and shorter mean length of stay (16.7 vs 32.1 days; <i>P</i> = .03). Median time to discharge was not statistically significant (6.4 vs 14.0 days; <i>P</i> = .17). The dual antipsychotic group had higher mean chlorpromazine equivalents (723 mg vs 356 mg; <i>P</i> = .002). There was no difference in 30-day readmission rates (16.7% vs 27.3%; χ<sup>2</sup> = 0.5765; <i>P</i> = .45).</p><p><strong>Discussion: </strong>This study found that following failure of antipsychotic monotherapy, transition to an alternative antipsychotic was associated with decreased mean time to discharge as compared to dual antipsychotic therapy. Further studies are needed to assess long-term clinical implications of these findings.</p>","PeriodicalId":22710,"journal":{"name":"The Mental Health Clinician","volume":"12 6","pages":"329-335"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/3c/a9/i2168-9709-12-6-329.PMC9819140.pdf","citationCount":"0","resultStr":"{\"title\":\"Comparison of antipsychotic prescribing practices following failure of antipsychotic monotherapy in the acute care setting.\",\"authors\":\"Kaitlyn Morgan, Leah Rickert\",\"doi\":\"10.9740/mhc.2022.12.329\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Numerous strategies exist following antipsychotic monotherapy failure including transition to another antipsychotic, dosing above FDA recommendations, or dual antipsychotic therapy. This study described antipsychotic prescribing practices on an acute psychiatry unit following antipsychotic monotherapy failure and compared outcomes to determine if any strategy resulted in superior short-term outcomes.</p><p><strong>Methods: </strong>This retrospective chart review assessed postintervention time to discharge for patients with schizophrenia or schizoaffective disorder requiring therapy change following treatment failure. Secondary outcomes included 30-day readmission rate, length of stay, and discharge chlorpromazine equivalents.</p><p><strong>Results: </strong>There were no differences in number of past antipsychotic trials between groups (4.8 vs 4.5; <i>P</i> = .73). Of all the patients, 73% (n = 30) discharged on alternative antipsychotic monotherapy while 27% (n = 11) discharged on dual antipsychotic therapy. No patients had doses increased above FDA recommendations. The alternative antipsychotic group had shorter mean postintervention time to discharge (8.8 vs 20.6 days; <i>P</i> = .003) and shorter mean length of stay (16.7 vs 32.1 days; <i>P</i> = .03). Median time to discharge was not statistically significant (6.4 vs 14.0 days; <i>P</i> = .17). The dual antipsychotic group had higher mean chlorpromazine equivalents (723 mg vs 356 mg; <i>P</i> = .002). There was no difference in 30-day readmission rates (16.7% vs 27.3%; χ<sup>2</sup> = 0.5765; <i>P</i> = .45).</p><p><strong>Discussion: </strong>This study found that following failure of antipsychotic monotherapy, transition to an alternative antipsychotic was associated with decreased mean time to discharge as compared to dual antipsychotic therapy. Further studies are needed to assess long-term clinical implications of these findings.</p>\",\"PeriodicalId\":22710,\"journal\":{\"name\":\"The Mental Health Clinician\",\"volume\":\"12 6\",\"pages\":\"329-335\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-01-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/3c/a9/i2168-9709-12-6-329.PMC9819140.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"The Mental Health Clinician\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.9740/mhc.2022.12.329\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/12/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Mental Health Clinician","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.9740/mhc.2022.12.329","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/12/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
简介:抗精神病药物单一疗法失败后有许多策略,包括过渡到另一种抗精神病药物、剂量高于FDA建议或双重抗精神病药物治疗。本研究描述了一个急性精神病科在抗精神病药单一疗法失败后的抗精神病药处方做法,并对结果进行了比较,以确定是否有哪种策略能带来更好的短期疗效:这项回顾性病历审查评估了治疗失败后需要更换治疗方案的精神分裂症或分裂情感障碍患者的干预后出院时间。次要结果包括 30 天再入院率、住院时间和出院氯丙嗪当量:两组患者既往抗精神病药物试验次数无差异(4.8 vs 4.5;P = .73)。在所有患者中,73%(n = 30)的患者出院时接受了替代性抗精神病药物单药治疗,27%(n = 11)的患者出院时接受了双重抗精神病药物治疗。没有患者的剂量增加超过美国食品药品管理局的建议。替代抗精神病药物组的干预后平均出院时间更短(8.8 天 vs 20.6 天;P = .003),平均住院时间更短(16.7 天 vs 32.1 天;P = .03)。中位出院时间无统计学意义(6.4 天 vs 14.0 天;P = .17)。双重抗精神病药物组的平均氯丙嗪当量更高(723 毫克 vs 356 毫克;P = .002)。30天再入院率没有差异(16.7% vs 27.3%;χ2 = 0.5765;P = .45):本研究发现,在单一抗精神病药物治疗失败后,与双重抗精神病药物治疗相比,转用其他抗精神病药物与平均出院时间缩短有关。还需要进一步的研究来评估这些发现的长期临床意义。
Comparison of antipsychotic prescribing practices following failure of antipsychotic monotherapy in the acute care setting.
Introduction: Numerous strategies exist following antipsychotic monotherapy failure including transition to another antipsychotic, dosing above FDA recommendations, or dual antipsychotic therapy. This study described antipsychotic prescribing practices on an acute psychiatry unit following antipsychotic monotherapy failure and compared outcomes to determine if any strategy resulted in superior short-term outcomes.
Methods: This retrospective chart review assessed postintervention time to discharge for patients with schizophrenia or schizoaffective disorder requiring therapy change following treatment failure. Secondary outcomes included 30-day readmission rate, length of stay, and discharge chlorpromazine equivalents.
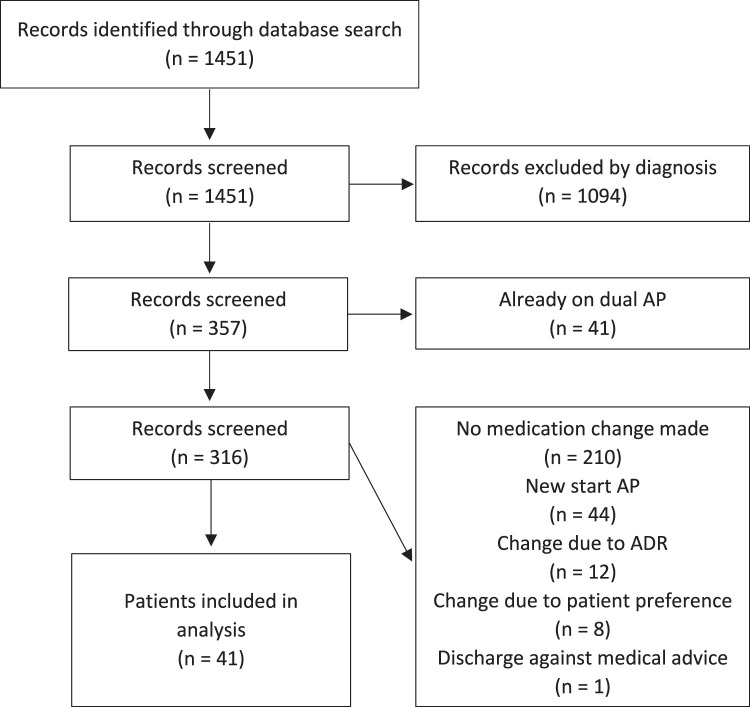
Results: There were no differences in number of past antipsychotic trials between groups (4.8 vs 4.5; P = .73). Of all the patients, 73% (n = 30) discharged on alternative antipsychotic monotherapy while 27% (n = 11) discharged on dual antipsychotic therapy. No patients had doses increased above FDA recommendations. The alternative antipsychotic group had shorter mean postintervention time to discharge (8.8 vs 20.6 days; P = .003) and shorter mean length of stay (16.7 vs 32.1 days; P = .03). Median time to discharge was not statistically significant (6.4 vs 14.0 days; P = .17). The dual antipsychotic group had higher mean chlorpromazine equivalents (723 mg vs 356 mg; P = .002). There was no difference in 30-day readmission rates (16.7% vs 27.3%; χ2 = 0.5765; P = .45).
Discussion: This study found that following failure of antipsychotic monotherapy, transition to an alternative antipsychotic was associated with decreased mean time to discharge as compared to dual antipsychotic therapy. Further studies are needed to assess long-term clinical implications of these findings.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


