{"title":"免疫抑制药物治疗的异体肾移植失败患者感染的危险因素。","authors":"Lauren Ogawa, Omer E Beaird, Joanna M Schaenman","doi":"10.3389/fneph.2023.1149116","DOIUrl":null,"url":null,"abstract":"<p><p>Patients with a failing kidney allograft are often continued on immunosuppression (IS) to preserve residual kidney function and prevent allosensitization. It has been previously accepted that maintaining patients on immunosuppressive therapy results in an increased risk of infection, hospitalization, and mortality. However, as the management of IS in patients with a failed kidney allograft continues to evolve, it is important to review the data regarding associations between infection and specific immunosuppression regimens. We present a review of the literature of failed kidney allograft management and infection risk, and discuss practices for infection prevention. Fifteen studies, published from 1995 to 2022, which investigated the experience of patients with failed allograft and infection, were identified. Infection was most commonly documented as a general event, but when specified, included infections caused by <i>Candida</i>, <i>Mycobacterium tuberculosis</i>, and <i>Aspergillus.</i> In addition, the definition of reduced \"IS\" varied from decreased doses of a triple drug regimen to monotherapy, whereas others did not specify which medications patients were receiving. Despite attempts at lowering net immunosuppression, patients with failed allografts remain at risk of acquiring opportunistic and non-opportunistic infections. Although opportunistic infections secondary to IS are expected, somewhat surprisingly, it appears that the greatest risk of infection may be related to complications of dialysis. Therefore, mitigating strategies, such as planning for an arteriovenous (AV) fistula over a hemodialysis catheter placement, may reduce infection risk. Additional studies are needed to provide more information regarding the types and timing of infection in the setting of a failed kidney allograft. In addition, more data are needed regarding specific medications, doses, and timing of taper of IS to guide future patient management and inform strategies for infection surveillance and prophylaxis.</p>","PeriodicalId":73091,"journal":{"name":"Frontiers in nephrology","volume":"3 ","pages":"1149116"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10479655/pdf/","citationCount":"0","resultStr":"{\"title\":\"Risk factors for infection in patients with a failed kidney allograft on immunosuppressive medications.\",\"authors\":\"Lauren Ogawa, Omer E Beaird, Joanna M Schaenman\",\"doi\":\"10.3389/fneph.2023.1149116\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Patients with a failing kidney allograft are often continued on immunosuppression (IS) to preserve residual kidney function and prevent allosensitization. It has been previously accepted that maintaining patients on immunosuppressive therapy results in an increased risk of infection, hospitalization, and mortality. However, as the management of IS in patients with a failed kidney allograft continues to evolve, it is important to review the data regarding associations between infection and specific immunosuppression regimens. We present a review of the literature of failed kidney allograft management and infection risk, and discuss practices for infection prevention. Fifteen studies, published from 1995 to 2022, which investigated the experience of patients with failed allograft and infection, were identified. Infection was most commonly documented as a general event, but when specified, included infections caused by <i>Candida</i>, <i>Mycobacterium tuberculosis</i>, and <i>Aspergillus.</i> In addition, the definition of reduced \\\"IS\\\" varied from decreased doses of a triple drug regimen to monotherapy, whereas others did not specify which medications patients were receiving. Despite attempts at lowering net immunosuppression, patients with failed allografts remain at risk of acquiring opportunistic and non-opportunistic infections. Although opportunistic infections secondary to IS are expected, somewhat surprisingly, it appears that the greatest risk of infection may be related to complications of dialysis. Therefore, mitigating strategies, such as planning for an arteriovenous (AV) fistula over a hemodialysis catheter placement, may reduce infection risk. Additional studies are needed to provide more information regarding the types and timing of infection in the setting of a failed kidney allograft. In addition, more data are needed regarding specific medications, doses, and timing of taper of IS to guide future patient management and inform strategies for infection surveillance and prophylaxis.</p>\",\"PeriodicalId\":73091,\"journal\":{\"name\":\"Frontiers in nephrology\",\"volume\":\"3 \",\"pages\":\"1149116\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10479655/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Frontiers in nephrology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3389/fneph.2023.1149116\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in nephrology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3389/fneph.2023.1149116","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Risk factors for infection in patients with a failed kidney allograft on immunosuppressive medications.
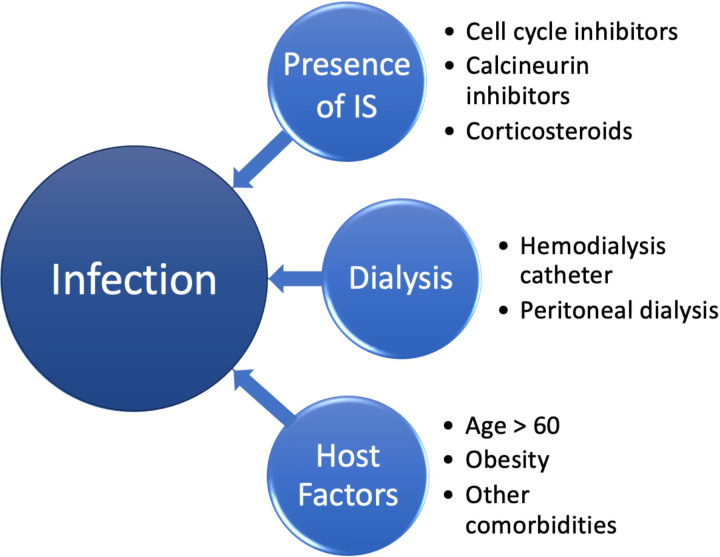
Patients with a failing kidney allograft are often continued on immunosuppression (IS) to preserve residual kidney function and prevent allosensitization. It has been previously accepted that maintaining patients on immunosuppressive therapy results in an increased risk of infection, hospitalization, and mortality. However, as the management of IS in patients with a failed kidney allograft continues to evolve, it is important to review the data regarding associations between infection and specific immunosuppression regimens. We present a review of the literature of failed kidney allograft management and infection risk, and discuss practices for infection prevention. Fifteen studies, published from 1995 to 2022, which investigated the experience of patients with failed allograft and infection, were identified. Infection was most commonly documented as a general event, but when specified, included infections caused by Candida, Mycobacterium tuberculosis, and Aspergillus. In addition, the definition of reduced "IS" varied from decreased doses of a triple drug regimen to monotherapy, whereas others did not specify which medications patients were receiving. Despite attempts at lowering net immunosuppression, patients with failed allografts remain at risk of acquiring opportunistic and non-opportunistic infections. Although opportunistic infections secondary to IS are expected, somewhat surprisingly, it appears that the greatest risk of infection may be related to complications of dialysis. Therefore, mitigating strategies, such as planning for an arteriovenous (AV) fistula over a hemodialysis catheter placement, may reduce infection risk. Additional studies are needed to provide more information regarding the types and timing of infection in the setting of a failed kidney allograft. In addition, more data are needed regarding specific medications, doses, and timing of taper of IS to guide future patient management and inform strategies for infection surveillance and prophylaxis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


