Arinze Nkemdirim Okere, Miquetta L Trimble, Vassiki Sanogo, Ukamaka Smith, Clyde Brown, Sarah G Buxbaum
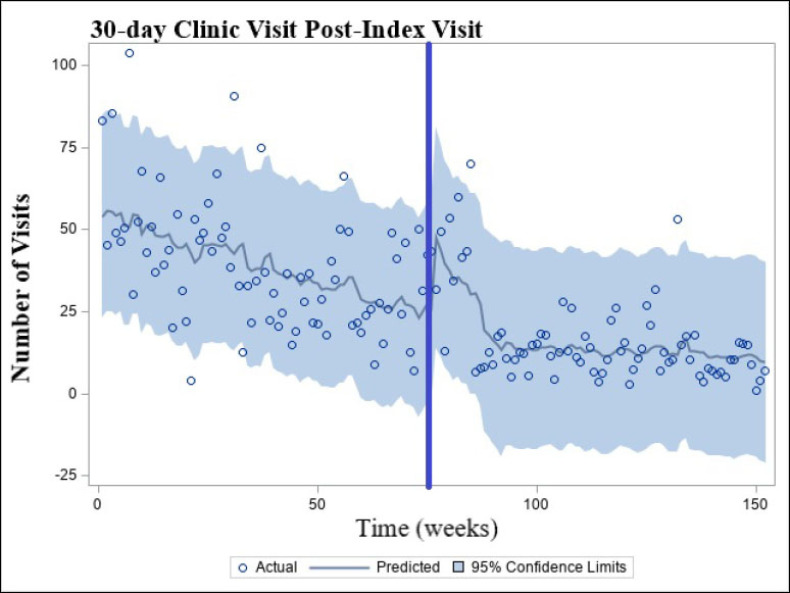
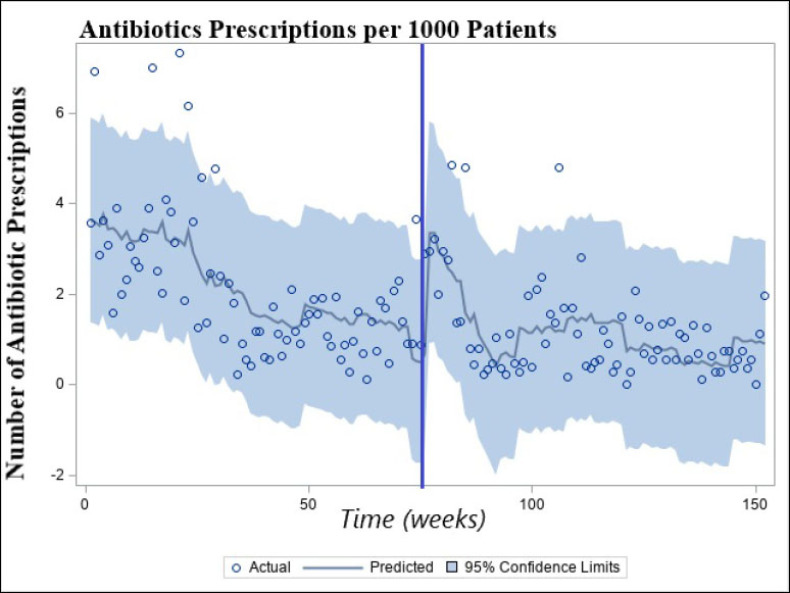
{"title":"通过将抗生素管理计划与低收入诊所的药物治疗服务相结合来实施抗生素管理计划的潜在影响-单中心体验。","authors":"Arinze Nkemdirim Okere, Miquetta L Trimble, Vassiki Sanogo, Ukamaka Smith, Clyde Brown, Sarah G Buxbaum","doi":"10.24926/iip.v13i3.4997","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Bacterial antimicrobial resistance (AMR) is a leading cause of mortality worldwide. Although AMR is common in low-income communities, there is limited evidence of the effect of antibiotic stewardship programs in low-income communities in the United States. <b>Objectives:</b> Our goal is to assess the effects of implementing pharmacist-led ASP by integrating it with medication therapy management service (MTM) in a low-income serving clinic. We evaluated the following 1) antibiotic prescriptions per 1000 patients, 2) the frequency of clinic (office) visits 30-day post-index clinic visits for recurring infections. <b>Methods:</b> To achieve our goal, we conducted a pre-post, quasi-experimental intervention study using an interrupted time-series analysis to assess the following: 1) antibiotic prescriptions per 1000 patients and the 2) frequency of office visits (including telehealth) within 30-day post-index clinic visits associated with recurrent infection. <b>Results:</b> Our findings revealed that the long-term effect of our antibiotic stewardship program intervention was associated with 63.69% reduction in antibiotic prescriptions per 1000 patients (change in slope = -0.173, [95% CI: (-0.30, -0.05)], P < 0.007) and a reduction in the frequency of office visits within 30-day post-index clinic visits by 67.27% (change in slope = -2.043, [95% CI: (-3.84, -0.24)], P < 0.028). <b>Conclusion:</b> Implementing antibiotic stewardship programs is feasible for clinics serving low-income populations. It was associated with a reduction in antibiotic prescriptions and preventable clinic (office) visits within 30 days due to infection recurrence.</p>","PeriodicalId":13646,"journal":{"name":"Innovations in Pharmacy","volume":"13 3","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/22/a2/21550417-13-03-4997.PMC9815868.pdf","citationCount":"0","resultStr":"{\"title\":\"The Potential Effects of Implementing an Antibiotic Stewardship Program by Integrating It with Medication Therapy Service in a Low-Income Serving Clinic - A Single-Center Experience.\",\"authors\":\"Arinze Nkemdirim Okere, Miquetta L Trimble, Vassiki Sanogo, Ukamaka Smith, Clyde Brown, Sarah G Buxbaum\",\"doi\":\"10.24926/iip.v13i3.4997\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background:</b> Bacterial antimicrobial resistance (AMR) is a leading cause of mortality worldwide. Although AMR is common in low-income communities, there is limited evidence of the effect of antibiotic stewardship programs in low-income communities in the United States. <b>Objectives:</b> Our goal is to assess the effects of implementing pharmacist-led ASP by integrating it with medication therapy management service (MTM) in a low-income serving clinic. We evaluated the following 1) antibiotic prescriptions per 1000 patients, 2) the frequency of clinic (office) visits 30-day post-index clinic visits for recurring infections. <b>Methods:</b> To achieve our goal, we conducted a pre-post, quasi-experimental intervention study using an interrupted time-series analysis to assess the following: 1) antibiotic prescriptions per 1000 patients and the 2) frequency of office visits (including telehealth) within 30-day post-index clinic visits associated with recurrent infection. <b>Results:</b> Our findings revealed that the long-term effect of our antibiotic stewardship program intervention was associated with 63.69% reduction in antibiotic prescriptions per 1000 patients (change in slope = -0.173, [95% CI: (-0.30, -0.05)], P < 0.007) and a reduction in the frequency of office visits within 30-day post-index clinic visits by 67.27% (change in slope = -2.043, [95% CI: (-3.84, -0.24)], P < 0.028). <b>Conclusion:</b> Implementing antibiotic stewardship programs is feasible for clinics serving low-income populations. It was associated with a reduction in antibiotic prescriptions and preventable clinic (office) visits within 30 days due to infection recurrence.</p>\",\"PeriodicalId\":13646,\"journal\":{\"name\":\"Innovations in Pharmacy\",\"volume\":\"13 3\",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/22/a2/21550417-13-03-4997.PMC9815868.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Innovations in Pharmacy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.24926/iip.v13i3.4997\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Innovations in Pharmacy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.24926/iip.v13i3.4997","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:细菌抗微生物药物耐药性(AMR)是世界范围内死亡的主要原因。虽然抗生素耐药性在低收入社区很常见,但美国低收入社区抗生素管理项目的效果证据有限。目的:我们的目标是通过将药师主导的ASP与药物治疗管理服务(MTM)相结合,评估在低收入服务诊所实施ASP的效果。我们评估了以下情况:1)每1000名患者的抗生素处方;2)在指数门诊就诊后30天的门诊(办公室)就诊频率。方法:为了实现我们的目标,我们使用中断时间序列分析进行了一项前后准实验干预研究,以评估以下内容:1)每1000名患者的抗生素处方,2)指数后30天内与复发感染相关的门诊就诊频率(包括远程医疗)。结果:我们的研究结果显示,我们的抗生素管理计划干预的长期效果与每1000名患者抗生素处方减少63.69%(斜率变化= -0.173,[95% CI: (-0.30, -0.05)], P < 0.007)和30天内诊所就诊频率减少67.27%(斜率变化= -2.043,[95% CI: (-3.84, -0.24)], P < 0.028)相关。结论:在低收入人群门诊实施抗生素管理方案是可行的。它与抗生素处方的减少和由于感染复发而在30天内可预防的诊所(办公室)就诊有关。
The Potential Effects of Implementing an Antibiotic Stewardship Program by Integrating It with Medication Therapy Service in a Low-Income Serving Clinic - A Single-Center Experience.
Background: Bacterial antimicrobial resistance (AMR) is a leading cause of mortality worldwide. Although AMR is common in low-income communities, there is limited evidence of the effect of antibiotic stewardship programs in low-income communities in the United States. Objectives: Our goal is to assess the effects of implementing pharmacist-led ASP by integrating it with medication therapy management service (MTM) in a low-income serving clinic. We evaluated the following 1) antibiotic prescriptions per 1000 patients, 2) the frequency of clinic (office) visits 30-day post-index clinic visits for recurring infections. Methods: To achieve our goal, we conducted a pre-post, quasi-experimental intervention study using an interrupted time-series analysis to assess the following: 1) antibiotic prescriptions per 1000 patients and the 2) frequency of office visits (including telehealth) within 30-day post-index clinic visits associated with recurrent infection. Results: Our findings revealed that the long-term effect of our antibiotic stewardship program intervention was associated with 63.69% reduction in antibiotic prescriptions per 1000 patients (change in slope = -0.173, [95% CI: (-0.30, -0.05)], P < 0.007) and a reduction in the frequency of office visits within 30-day post-index clinic visits by 67.27% (change in slope = -2.043, [95% CI: (-3.84, -0.24)], P < 0.028). Conclusion: Implementing antibiotic stewardship programs is feasible for clinics serving low-income populations. It was associated with a reduction in antibiotic prescriptions and preventable clinic (office) visits within 30 days due to infection recurrence.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


