Binoy Yohannan, Allen C Omo-Ogboi, Varaha S Tammisetti, Adan Rios
{"title":"自身免疫性肝炎和多发性骨髓瘤的同步表现","authors":"Binoy Yohannan, Allen C Omo-Ogboi, Varaha S Tammisetti, Adan Rios","doi":"10.14740/jh1049","DOIUrl":null,"url":null,"abstract":"<p><p>Autoimmune hepatitis (AIH) is a rare immune-mediated disease predominantly seen in women and triggered by various environmental factors. Rarely, AIH can be triggered by an underlying malignancy. We report a woman in her 60s who presented with markedly abnormal liver biochemical tests. Serology was positive for anti-smooth muscle antibodies and a liver biopsy confirmed AIH. During the hospital course, she developed sepsis and acute renal failure requiring dialysis support. Serum protein electrophoresis (SPEP) showed a monoclonal IgG kappa protein of 1.92 g/dL and a bone marrow biopsy revealed 7% clonal plasma cells. She had lytic lesions on skeletal survey confirming the diagnosis of a coexisting multiple myeloma (MM). Given her markedly abnormal liver chemistries, we decided to treat the AIH first and use the steroids (an important anti-myeloma therapy) as a bridge to the specific treatment of the MM once her clinical condition improved. She was treated with oral prednisone and azathioprine for AIH. One month later, a marked improvement in liver biochemical test results was noted and she was started on oral ixazomib, lenalidomide and dexamethasone. She received palliative radiotherapy to the lumbar spine (L2), left femur, and ischium lesions. This case highlights a rare co-occurrence of AIH and MM, the underlying mechanism of which is unknown.</p>","PeriodicalId":15964,"journal":{"name":"Journal of hematology","volume":"11 6","pages":"216-222"},"PeriodicalIF":1.3000,"publicationDate":"2022-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/8f/e2/jh-11-216.PMC9822655.pdf","citationCount":"0","resultStr":"{\"title\":\"Synchronous Presentation of Autoimmune Hepatitis and Multiple Myeloma.\",\"authors\":\"Binoy Yohannan, Allen C Omo-Ogboi, Varaha S Tammisetti, Adan Rios\",\"doi\":\"10.14740/jh1049\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Autoimmune hepatitis (AIH) is a rare immune-mediated disease predominantly seen in women and triggered by various environmental factors. Rarely, AIH can be triggered by an underlying malignancy. We report a woman in her 60s who presented with markedly abnormal liver biochemical tests. Serology was positive for anti-smooth muscle antibodies and a liver biopsy confirmed AIH. During the hospital course, she developed sepsis and acute renal failure requiring dialysis support. Serum protein electrophoresis (SPEP) showed a monoclonal IgG kappa protein of 1.92 g/dL and a bone marrow biopsy revealed 7% clonal plasma cells. She had lytic lesions on skeletal survey confirming the diagnosis of a coexisting multiple myeloma (MM). Given her markedly abnormal liver chemistries, we decided to treat the AIH first and use the steroids (an important anti-myeloma therapy) as a bridge to the specific treatment of the MM once her clinical condition improved. She was treated with oral prednisone and azathioprine for AIH. One month later, a marked improvement in liver biochemical test results was noted and she was started on oral ixazomib, lenalidomide and dexamethasone. She received palliative radiotherapy to the lumbar spine (L2), left femur, and ischium lesions. This case highlights a rare co-occurrence of AIH and MM, the underlying mechanism of which is unknown.</p>\",\"PeriodicalId\":15964,\"journal\":{\"name\":\"Journal of hematology\",\"volume\":\"11 6\",\"pages\":\"216-222\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2022-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/8f/e2/jh-11-216.PMC9822655.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of hematology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14740/jh1049\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of hematology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/jh1049","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"HEMATOLOGY","Score":null,"Total":0}
Synchronous Presentation of Autoimmune Hepatitis and Multiple Myeloma.
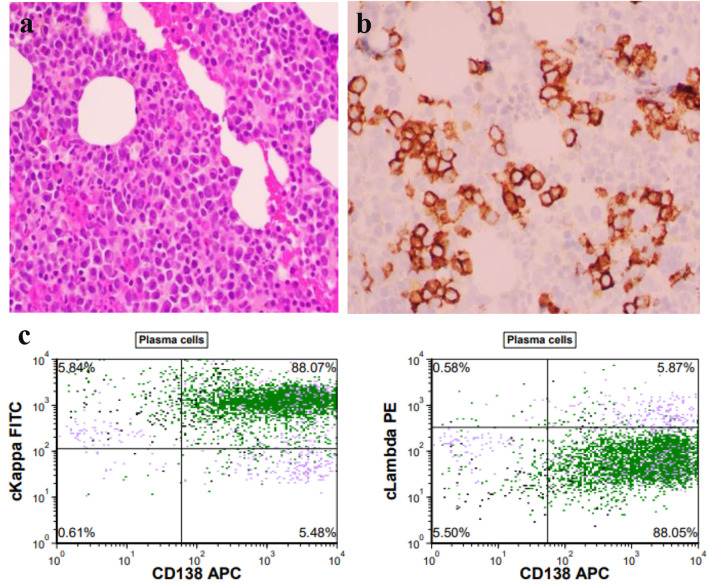
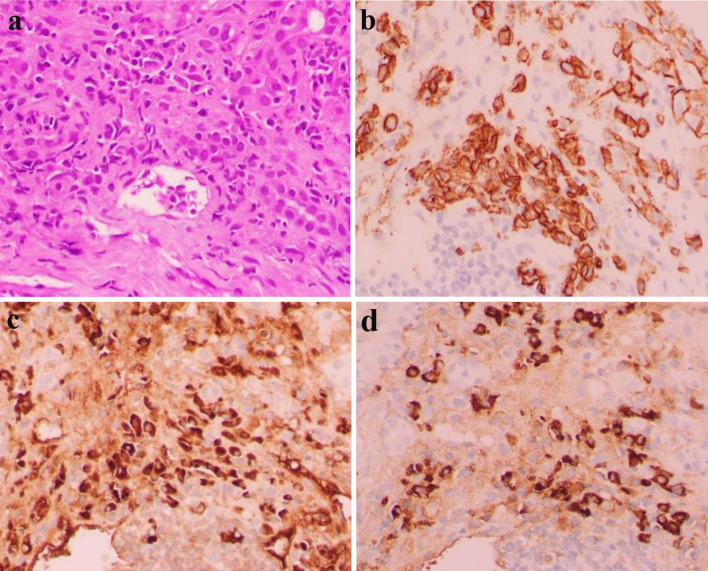
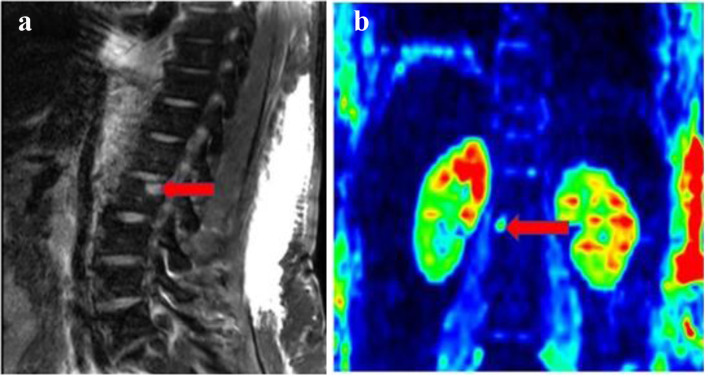
Autoimmune hepatitis (AIH) is a rare immune-mediated disease predominantly seen in women and triggered by various environmental factors. Rarely, AIH can be triggered by an underlying malignancy. We report a woman in her 60s who presented with markedly abnormal liver biochemical tests. Serology was positive for anti-smooth muscle antibodies and a liver biopsy confirmed AIH. During the hospital course, she developed sepsis and acute renal failure requiring dialysis support. Serum protein electrophoresis (SPEP) showed a monoclonal IgG kappa protein of 1.92 g/dL and a bone marrow biopsy revealed 7% clonal plasma cells. She had lytic lesions on skeletal survey confirming the diagnosis of a coexisting multiple myeloma (MM). Given her markedly abnormal liver chemistries, we decided to treat the AIH first and use the steroids (an important anti-myeloma therapy) as a bridge to the specific treatment of the MM once her clinical condition improved. She was treated with oral prednisone and azathioprine for AIH. One month later, a marked improvement in liver biochemical test results was noted and she was started on oral ixazomib, lenalidomide and dexamethasone. She received palliative radiotherapy to the lumbar spine (L2), left femur, and ischium lesions. This case highlights a rare co-occurrence of AIH and MM, the underlying mechanism of which is unknown.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


