{"title":"撒哈拉以南非洲已婚妇女未满足的计划生育需求:1995 - 2020年人口健康调查数据的荟萃分析。","authors":"Million Phiri, Clifford Odimegwu, Chester Kalinda","doi":"10.1186/s40834-022-00198-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Closing the gap of unmet needs for family planning (FP) in sub-Saharan Africa remains critical in improving maternal and child health outcomes. Determining the prevalence of unmet needs for family planning among married women in the reproductive age is vital for designing effective sexual reproductive health interventions and programmes. Here, we use nationally representative data drawn from sub-Saharan countries to estimate and examine heterogeneity of unmet needs for family planning among currently married women of reproductive age.</p><p><strong>Methods: </strong>This study used secondary data from Demographic and Health Surveys (DHS) conducted between January 1, 1995 to December 31, 2020 from 37 countries in sub-Saharan African. An Inverse Heterogeneity model (IVhet) in MetaXL application was used to estimate country and sub-regional level pooled estimates and confidence intervals of unmet needs for FP in SSA.</p><p><strong>Results: </strong>The overall prevalence of unmet need for family planning among married women of reproductive age in the sub-region for the period under study was 22.9% (95% CI: 20.9-25.0). The prevalence varied across countries from 10% (95% CI: 10-11%) in Zimbabwe to 38% (95% CI: 35-40) and 38 (95% CI: 37-39) (I2 = 99.8% and p-value < 0.0001) in Sao Tome and Principe and Angola, respectively. Unmet needs due to limiting ranged from 6%; (95% CI: 3-9) in Central Africa to 9%; (95% CI: 8-11) in East Africa. On the other hand, the prevalence of unmet needs due to spacing was highest in Central Africa (Prev: 18; 95% CI: 16-21) and lowest in Southern Africa (Prev: 12%; 95% CI: 8-16). Our study indicates that there was no publication bias because the Luis Furuya-Kanamori index (0.79) was within the symmetry range of -1 and + 1.</p><p><strong>Conclusion: </strong>The prevalence of unmet need for FP remains high in sub-Saharan Africa suggesting the need for health policymakers to consider re-evaluating the current SRH policies and programmes with the view of redesigning the present successful strategies to address the problem.</p>","PeriodicalId":10637,"journal":{"name":"Contraception and Reproductive Medicine","volume":"8 1","pages":"3"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9832678/pdf/","citationCount":"2","resultStr":"{\"title\":\"Unmet need for family planning among married women in sub-Saharan Africa: a meta-analysis of DHS data (1995 - 2020).\",\"authors\":\"Million Phiri, Clifford Odimegwu, Chester Kalinda\",\"doi\":\"10.1186/s40834-022-00198-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Closing the gap of unmet needs for family planning (FP) in sub-Saharan Africa remains critical in improving maternal and child health outcomes. Determining the prevalence of unmet needs for family planning among married women in the reproductive age is vital for designing effective sexual reproductive health interventions and programmes. Here, we use nationally representative data drawn from sub-Saharan countries to estimate and examine heterogeneity of unmet needs for family planning among currently married women of reproductive age.</p><p><strong>Methods: </strong>This study used secondary data from Demographic and Health Surveys (DHS) conducted between January 1, 1995 to December 31, 2020 from 37 countries in sub-Saharan African. An Inverse Heterogeneity model (IVhet) in MetaXL application was used to estimate country and sub-regional level pooled estimates and confidence intervals of unmet needs for FP in SSA.</p><p><strong>Results: </strong>The overall prevalence of unmet need for family planning among married women of reproductive age in the sub-region for the period under study was 22.9% (95% CI: 20.9-25.0). The prevalence varied across countries from 10% (95% CI: 10-11%) in Zimbabwe to 38% (95% CI: 35-40) and 38 (95% CI: 37-39) (I2 = 99.8% and p-value < 0.0001) in Sao Tome and Principe and Angola, respectively. Unmet needs due to limiting ranged from 6%; (95% CI: 3-9) in Central Africa to 9%; (95% CI: 8-11) in East Africa. On the other hand, the prevalence of unmet needs due to spacing was highest in Central Africa (Prev: 18; 95% CI: 16-21) and lowest in Southern Africa (Prev: 12%; 95% CI: 8-16). Our study indicates that there was no publication bias because the Luis Furuya-Kanamori index (0.79) was within the symmetry range of -1 and + 1.</p><p><strong>Conclusion: </strong>The prevalence of unmet need for FP remains high in sub-Saharan Africa suggesting the need for health policymakers to consider re-evaluating the current SRH policies and programmes with the view of redesigning the present successful strategies to address the problem.</p>\",\"PeriodicalId\":10637,\"journal\":{\"name\":\"Contraception and Reproductive Medicine\",\"volume\":\"8 1\",\"pages\":\"3\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-01-11\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9832678/pdf/\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Contraception and Reproductive Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s40834-022-00198-5\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Contraception and Reproductive Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40834-022-00198-5","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Unmet need for family planning among married women in sub-Saharan Africa: a meta-analysis of DHS data (1995 - 2020).
Background: Closing the gap of unmet needs for family planning (FP) in sub-Saharan Africa remains critical in improving maternal and child health outcomes. Determining the prevalence of unmet needs for family planning among married women in the reproductive age is vital for designing effective sexual reproductive health interventions and programmes. Here, we use nationally representative data drawn from sub-Saharan countries to estimate and examine heterogeneity of unmet needs for family planning among currently married women of reproductive age.
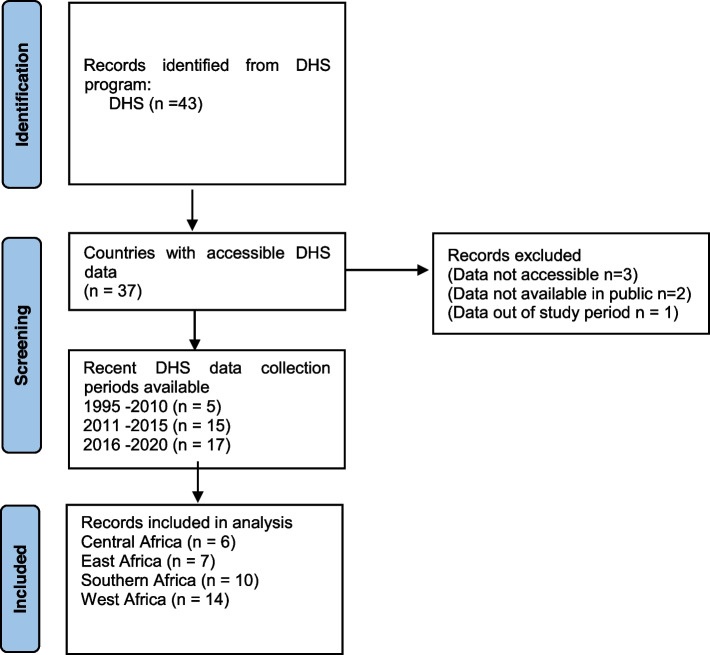
Methods: This study used secondary data from Demographic and Health Surveys (DHS) conducted between January 1, 1995 to December 31, 2020 from 37 countries in sub-Saharan African. An Inverse Heterogeneity model (IVhet) in MetaXL application was used to estimate country and sub-regional level pooled estimates and confidence intervals of unmet needs for FP in SSA.
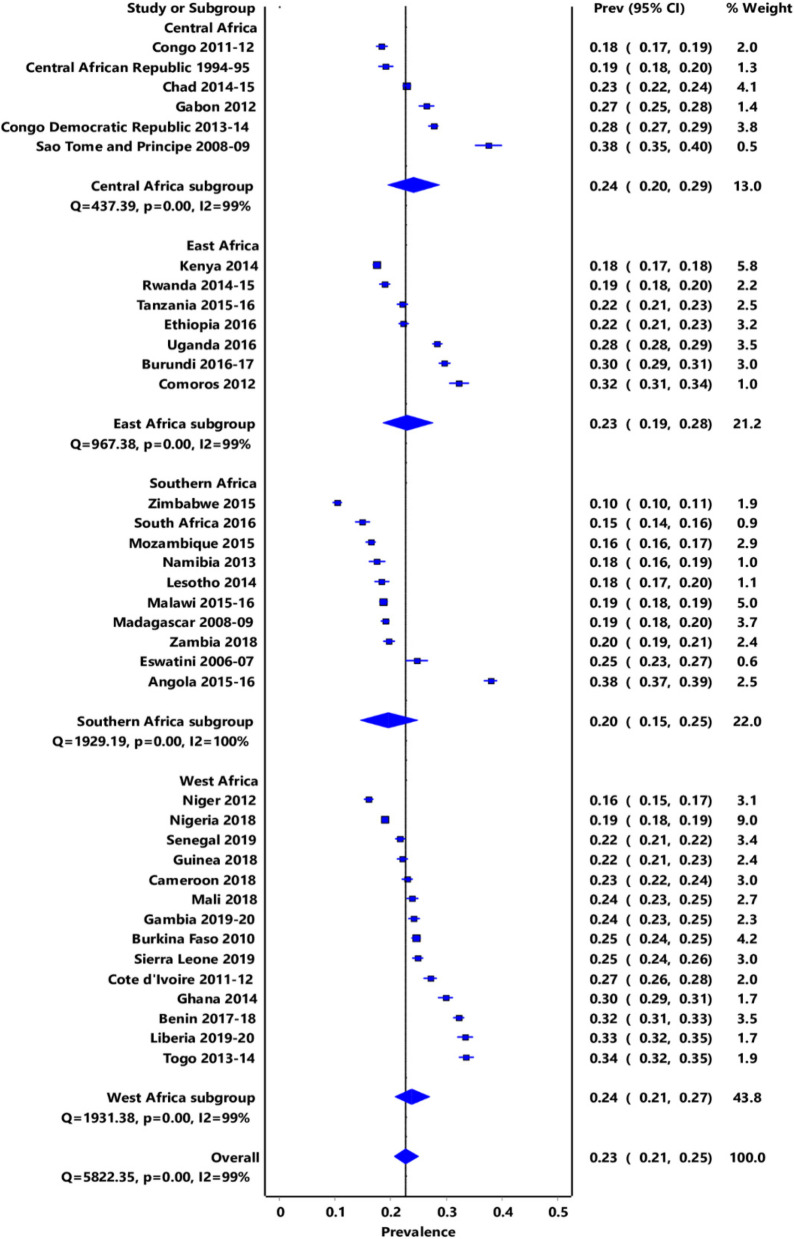
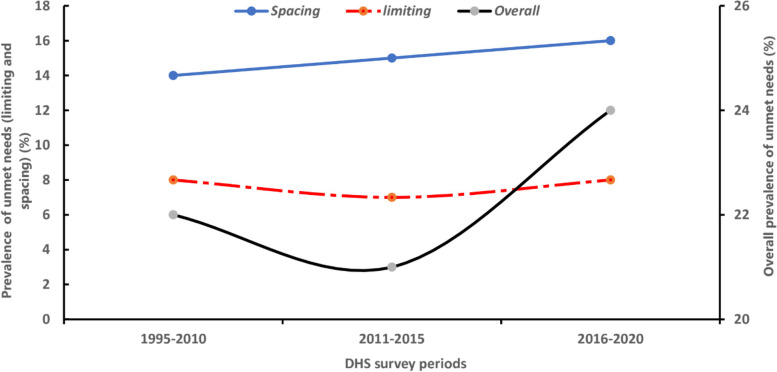
Results: The overall prevalence of unmet need for family planning among married women of reproductive age in the sub-region for the period under study was 22.9% (95% CI: 20.9-25.0). The prevalence varied across countries from 10% (95% CI: 10-11%) in Zimbabwe to 38% (95% CI: 35-40) and 38 (95% CI: 37-39) (I2 = 99.8% and p-value < 0.0001) in Sao Tome and Principe and Angola, respectively. Unmet needs due to limiting ranged from 6%; (95% CI: 3-9) in Central Africa to 9%; (95% CI: 8-11) in East Africa. On the other hand, the prevalence of unmet needs due to spacing was highest in Central Africa (Prev: 18; 95% CI: 16-21) and lowest in Southern Africa (Prev: 12%; 95% CI: 8-16). Our study indicates that there was no publication bias because the Luis Furuya-Kanamori index (0.79) was within the symmetry range of -1 and + 1.
Conclusion: The prevalence of unmet need for FP remains high in sub-Saharan Africa suggesting the need for health policymakers to consider re-evaluating the current SRH policies and programmes with the view of redesigning the present successful strategies to address the problem.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


