{"title":"连续小剂量阿司匹林在显微内镜椎板切除术中的安全性和临床效果。","authors":"Kiyoshi Tarukado, Teruaki Ono, Toshio Doi, Katsumi Harimaya, Yasuharu Nakashima","doi":"10.22603/ssrr.2022-0224","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>It remains controversial whether it is better to continue oral low-dose aspirin (LDA) during the perioperative period in spinal surgery. This study aims to evaluate the safety of continued LDA administration in the perioperative periods of microendoscopic laminectomy (MEL) by assessing perioperative complications and clinical outcomes.</p><p><strong>Methods: </strong>We ultimately included 88 patients (35 males, 53 females) who underwent one level of MEL for lumbar spinal canal stenosis from April 2016 to March 2022. Patients who did not undergo anticoagulation therapy were classified into Group A (65 patients), those who stopped anticoagulation therapy at the perioperative periods were classified into Group B (9 patients), and those who continued oral administration of LDA throughout the perioperative periods were classified into Group C (14 patients). Surgery time, intraoperative estimate blood loss (EBL), differences between hemoglobin (Hb) and platelet (Plt) before and after surgery, perioperative complications, and cross-sectional area of hematoma and dural sac on MRI taken within 1 week and at 6 months or more after surgery were assessed between three groups. The EuroQol-5 dimensions (EQ-5D), Oswestry Disability Index (ODI), and Japanese Orthopaedic Association Back Pain Evaluation Questionnaire (JOABPEQ) were also evaluated as the clinical outcomes.</p><p><strong>Results: </strong>There was no statistically significant difference between the three groups in operation time, intraoperative EBL, differences between Hb and Plt before and after surgery, and cross-sectional area of hematoma and dural sac on MRI. A case of hematoma removal was confirmed in Group A. There was also no statistically significant difference between the three groups in EQ-5D, ODI, and each domain of JOABPEQ.</p><p><strong>Conclusions: </strong>The continuation of LDA throughout the perioperative periods did not affect perioperative complications and clinical outcomes of one-level MEL. In MEL, it might be possible to continue oral administration of LDA throughout the perioperative periods.</p>","PeriodicalId":22253,"journal":{"name":"Spine Surgery and Related Research","volume":"7 4","pages":"350-355"},"PeriodicalIF":1.2000,"publicationDate":"2023-07-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/68/4c/2432-261X-7-0350.PMC10447200.pdf","citationCount":"0","resultStr":"{\"title\":\"Safety and Clinical Results of Continuous Low-Dose Aspirin in Microendoscopic Laminectomy.\",\"authors\":\"Kiyoshi Tarukado, Teruaki Ono, Toshio Doi, Katsumi Harimaya, Yasuharu Nakashima\",\"doi\":\"10.22603/ssrr.2022-0224\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>It remains controversial whether it is better to continue oral low-dose aspirin (LDA) during the perioperative period in spinal surgery. This study aims to evaluate the safety of continued LDA administration in the perioperative periods of microendoscopic laminectomy (MEL) by assessing perioperative complications and clinical outcomes.</p><p><strong>Methods: </strong>We ultimately included 88 patients (35 males, 53 females) who underwent one level of MEL for lumbar spinal canal stenosis from April 2016 to March 2022. Patients who did not undergo anticoagulation therapy were classified into Group A (65 patients), those who stopped anticoagulation therapy at the perioperative periods were classified into Group B (9 patients), and those who continued oral administration of LDA throughout the perioperative periods were classified into Group C (14 patients). Surgery time, intraoperative estimate blood loss (EBL), differences between hemoglobin (Hb) and platelet (Plt) before and after surgery, perioperative complications, and cross-sectional area of hematoma and dural sac on MRI taken within 1 week and at 6 months or more after surgery were assessed between three groups. The EuroQol-5 dimensions (EQ-5D), Oswestry Disability Index (ODI), and Japanese Orthopaedic Association Back Pain Evaluation Questionnaire (JOABPEQ) were also evaluated as the clinical outcomes.</p><p><strong>Results: </strong>There was no statistically significant difference between the three groups in operation time, intraoperative EBL, differences between Hb and Plt before and after surgery, and cross-sectional area of hematoma and dural sac on MRI. A case of hematoma removal was confirmed in Group A. There was also no statistically significant difference between the three groups in EQ-5D, ODI, and each domain of JOABPEQ.</p><p><strong>Conclusions: </strong>The continuation of LDA throughout the perioperative periods did not affect perioperative complications and clinical outcomes of one-level MEL. In MEL, it might be possible to continue oral administration of LDA throughout the perioperative periods.</p>\",\"PeriodicalId\":22253,\"journal\":{\"name\":\"Spine Surgery and Related Research\",\"volume\":\"7 4\",\"pages\":\"350-355\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2023-07-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/68/4c/2432-261X-7-0350.PMC10447200.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Spine Surgery and Related Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.22603/ssrr.2022-0224\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Spine Surgery and Related Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22603/ssrr.2022-0224","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
Safety and Clinical Results of Continuous Low-Dose Aspirin in Microendoscopic Laminectomy.
Introduction: It remains controversial whether it is better to continue oral low-dose aspirin (LDA) during the perioperative period in spinal surgery. This study aims to evaluate the safety of continued LDA administration in the perioperative periods of microendoscopic laminectomy (MEL) by assessing perioperative complications and clinical outcomes.
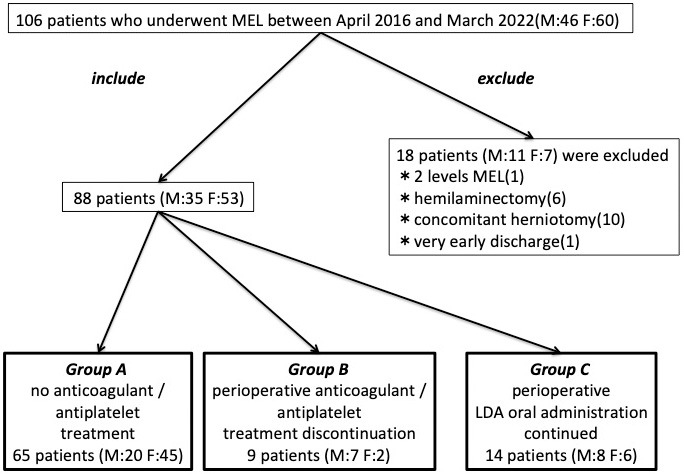
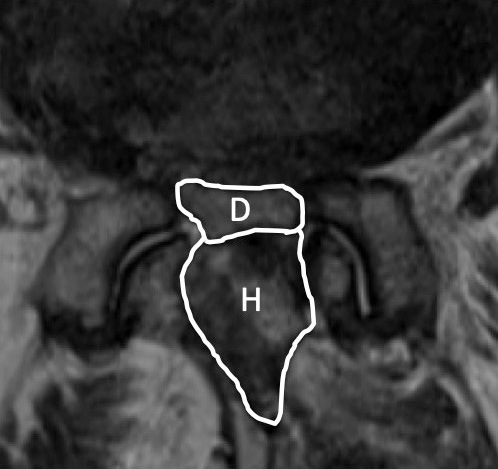
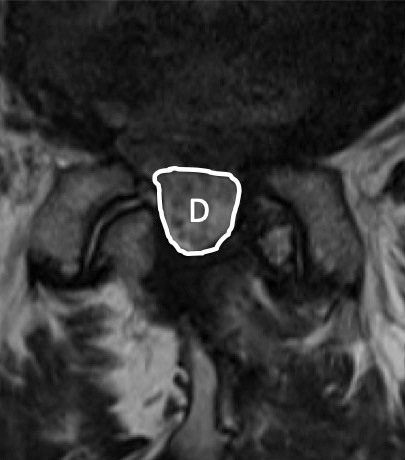
Methods: We ultimately included 88 patients (35 males, 53 females) who underwent one level of MEL for lumbar spinal canal stenosis from April 2016 to March 2022. Patients who did not undergo anticoagulation therapy were classified into Group A (65 patients), those who stopped anticoagulation therapy at the perioperative periods were classified into Group B (9 patients), and those who continued oral administration of LDA throughout the perioperative periods were classified into Group C (14 patients). Surgery time, intraoperative estimate blood loss (EBL), differences between hemoglobin (Hb) and platelet (Plt) before and after surgery, perioperative complications, and cross-sectional area of hematoma and dural sac on MRI taken within 1 week and at 6 months or more after surgery were assessed between three groups. The EuroQol-5 dimensions (EQ-5D), Oswestry Disability Index (ODI), and Japanese Orthopaedic Association Back Pain Evaluation Questionnaire (JOABPEQ) were also evaluated as the clinical outcomes.
Results: There was no statistically significant difference between the three groups in operation time, intraoperative EBL, differences between Hb and Plt before and after surgery, and cross-sectional area of hematoma and dural sac on MRI. A case of hematoma removal was confirmed in Group A. There was also no statistically significant difference between the three groups in EQ-5D, ODI, and each domain of JOABPEQ.
Conclusions: The continuation of LDA throughout the perioperative periods did not affect perioperative complications and clinical outcomes of one-level MEL. In MEL, it might be possible to continue oral administration of LDA throughout the perioperative periods.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


