{"title":"中央浆液性脉络膜视网膜病变继发于渗出性视网膜脱离1例。","authors":"Ji Young Moon, Se Joon Woo, Soo Chang Cho","doi":"10.3341/kjo.2022.0099","DOIUrl":null,"url":null,"abstract":"Dear Editor, Bullous central serous chorioretinopathy (bCSC) is an atypical variant of CSC, characterized by exudative retinal detachment, especially in inferior quadrants [1]. Subretinal pigment epithelium (sub-RPE) fibrin and increased hydrostatic pressure in pigment epithelial detachment (PED) is speculated to induce a RPE tear [2]. Subsequently, intense accumulation of subretinal fluid (SRF) leads to exudative retinal detachment. Proper treatment choice for bCSC is unclear. Removal of risk factors, focal laser, photodynamic therapy (PDT), and surgery can be applied [2]. There are two methods for surgical draining SRF: internal and external approach. Internal drainage may lead to retinotomy-associated rhegmatogenous retinal detachment (RD) [3]. Pars plana vitrectomy (PPV) with external drainage does not need retinotomy, allowing laser photocoagulation with an improved view using perfluorocarbon liquid (PFCL) and immediate retinal reattachment [4]. We report a case of bCSC treated with external drainage and vitrectomy in which the retina was reattached and maintained without recurrence for more than 1.5 years. Informed consent was obtained from the patient for publication of this case report and relevant images. A 51-year-old male patient presented with blurred vision in his right eye that started 5 days ago. Uncorrected visual acuity was 20 / 20, and intraocular pressure was normal in both eyes. Anterior segment was unremarkable. Fundus showed inferior bullous RD and no breaks in the right eye (Fig. 1A). Fundus was normal in the left eye. Perifoveal PEDs were found in the right eye (Fig. 1B). SRF increased the day after admission (Fig. 1C, 1D). Fluorescein angiography showed multiple perifoveal leaking points, a main inferonasal leaking point, and consequent pooling to the subretinal space (Fig. 1E, 1F). Optical coherence tomography (OCT) showed RPE tear at the site corresponding to the main leaking point (Fig. 1G). Exudative RD secondary to CSC (i.e., bCSC) was diagnosed and laser photocoagulation at leaking points was performed. On the 3rd day of admission, best-corrected visual acuity (BCVA) was 20 / 40, fundus showed shifting of SRF after sleeping on one side (Fig. 1H). Indocyanine green angiography shows hyper-permeable and dilated choroidal vessels (Fig. 1I). SRF decreased in OCT (Fig. 1J). He was discharged on the 5th day of admission. However, SRF increased significantly, and BCVA was 20 / 67 at outpatient visit at 5 days after discharge. We decided to transfer him for PDT. The next day, he was transferred to another hospital. BCVA decreased to finger count. Exudative RD was extended and prominent (Fig. 1K, 1L). Therefore, PDT was considered ineffective. After waiting 1 week, RD was further extended, and surgery was performed by SJW (Fig. 1M-1O). External drainage, PPV with perfluorocarbon liquid, endolaser, and intravitreal sulfur hexafluoride 18% gas injection were performed (Supplementary Video 1). Three months after surgery, BCVA was 20 / 40 and fundus showed flat retina and laser markings at nasal midperiphery (Fig. 1P, 1Q). One year and 8 months after surgery, BCVA was 20 / 29 and fundus was flat (Fig. 1R, 1S). To the best of our knowledge, this is the first report of bCSC successfully treated with external drainage and vitrectomy in Korea. Kang et al. [5] presented bilateral bCSC treated with internal drainage and vitrectomy. Their patient was initially treated with corticosteroid under diagnosis of Vogt–Koyanagi–Harada. Despite focal laser, exudative RD extended to fovea. External drainage, intravitreal gas injection, scleral buckling, and focal laser were applied. After 2 months, internal drainage, PPV, intravitreal gas injection, and focal laser were performed for recurrent RD [5]. In contrast, in our case, retina was attached and remained without recurrence during about 1.5 years after external drainage. In the study by Kang et al. [5], initial surKorean J Ophthalmol 2022;36(6):575-577 https://doi.org/10.3341/kjo.2022.0099","PeriodicalId":17883,"journal":{"name":"Korean Journal of Ophthalmology : KJO","volume":"36 6","pages":"575-577"},"PeriodicalIF":0.0000,"publicationDate":"2022-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/7f/0d/kjo-2022-0099.PMC9745348.pdf","citationCount":"0","resultStr":"{\"title\":\"External Subretinal Fluid Drainage and Vitrectomy in Exudative Retinal Detachment Secondary to Central Serous Chorioretinopathy: A Case Report.\",\"authors\":\"Ji Young Moon, Se Joon Woo, Soo Chang Cho\",\"doi\":\"10.3341/kjo.2022.0099\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"Dear Editor, Bullous central serous chorioretinopathy (bCSC) is an atypical variant of CSC, characterized by exudative retinal detachment, especially in inferior quadrants [1]. Subretinal pigment epithelium (sub-RPE) fibrin and increased hydrostatic pressure in pigment epithelial detachment (PED) is speculated to induce a RPE tear [2]. Subsequently, intense accumulation of subretinal fluid (SRF) leads to exudative retinal detachment. Proper treatment choice for bCSC is unclear. Removal of risk factors, focal laser, photodynamic therapy (PDT), and surgery can be applied [2]. There are two methods for surgical draining SRF: internal and external approach. Internal drainage may lead to retinotomy-associated rhegmatogenous retinal detachment (RD) [3]. Pars plana vitrectomy (PPV) with external drainage does not need retinotomy, allowing laser photocoagulation with an improved view using perfluorocarbon liquid (PFCL) and immediate retinal reattachment [4]. We report a case of bCSC treated with external drainage and vitrectomy in which the retina was reattached and maintained without recurrence for more than 1.5 years. Informed consent was obtained from the patient for publication of this case report and relevant images. A 51-year-old male patient presented with blurred vision in his right eye that started 5 days ago. Uncorrected visual acuity was 20 / 20, and intraocular pressure was normal in both eyes. Anterior segment was unremarkable. Fundus showed inferior bullous RD and no breaks in the right eye (Fig. 1A). Fundus was normal in the left eye. Perifoveal PEDs were found in the right eye (Fig. 1B). SRF increased the day after admission (Fig. 1C, 1D). Fluorescein angiography showed multiple perifoveal leaking points, a main inferonasal leaking point, and consequent pooling to the subretinal space (Fig. 1E, 1F). Optical coherence tomography (OCT) showed RPE tear at the site corresponding to the main leaking point (Fig. 1G). Exudative RD secondary to CSC (i.e., bCSC) was diagnosed and laser photocoagulation at leaking points was performed. On the 3rd day of admission, best-corrected visual acuity (BCVA) was 20 / 40, fundus showed shifting of SRF after sleeping on one side (Fig. 1H). Indocyanine green angiography shows hyper-permeable and dilated choroidal vessels (Fig. 1I). SRF decreased in OCT (Fig. 1J). He was discharged on the 5th day of admission. However, SRF increased significantly, and BCVA was 20 / 67 at outpatient visit at 5 days after discharge. We decided to transfer him for PDT. The next day, he was transferred to another hospital. BCVA decreased to finger count. Exudative RD was extended and prominent (Fig. 1K, 1L). Therefore, PDT was considered ineffective. After waiting 1 week, RD was further extended, and surgery was performed by SJW (Fig. 1M-1O). External drainage, PPV with perfluorocarbon liquid, endolaser, and intravitreal sulfur hexafluoride 18% gas injection were performed (Supplementary Video 1). Three months after surgery, BCVA was 20 / 40 and fundus showed flat retina and laser markings at nasal midperiphery (Fig. 1P, 1Q). One year and 8 months after surgery, BCVA was 20 / 29 and fundus was flat (Fig. 1R, 1S). To the best of our knowledge, this is the first report of bCSC successfully treated with external drainage and vitrectomy in Korea. Kang et al. [5] presented bilateral bCSC treated with internal drainage and vitrectomy. Their patient was initially treated with corticosteroid under diagnosis of Vogt–Koyanagi–Harada. Despite focal laser, exudative RD extended to fovea. External drainage, intravitreal gas injection, scleral buckling, and focal laser were applied. After 2 months, internal drainage, PPV, intravitreal gas injection, and focal laser were performed for recurrent RD [5]. In contrast, in our case, retina was attached and remained without recurrence during about 1.5 years after external drainage. In the study by Kang et al. [5], initial surKorean J Ophthalmol 2022;36(6):575-577 https://doi.org/10.3341/kjo.2022.0099\",\"PeriodicalId\":17883,\"journal\":{\"name\":\"Korean Journal of Ophthalmology : KJO\",\"volume\":\"36 6\",\"pages\":\"575-577\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/7f/0d/kjo-2022-0099.PMC9745348.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Korean Journal of Ophthalmology : KJO\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3341/kjo.2022.0099\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Korean Journal of Ophthalmology : KJO","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3341/kjo.2022.0099","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
External Subretinal Fluid Drainage and Vitrectomy in Exudative Retinal Detachment Secondary to Central Serous Chorioretinopathy: A Case Report.
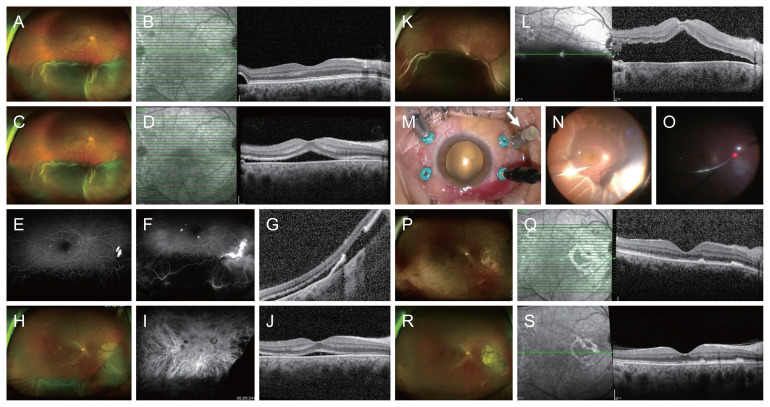
Dear Editor, Bullous central serous chorioretinopathy (bCSC) is an atypical variant of CSC, characterized by exudative retinal detachment, especially in inferior quadrants [1]. Subretinal pigment epithelium (sub-RPE) fibrin and increased hydrostatic pressure in pigment epithelial detachment (PED) is speculated to induce a RPE tear [2]. Subsequently, intense accumulation of subretinal fluid (SRF) leads to exudative retinal detachment. Proper treatment choice for bCSC is unclear. Removal of risk factors, focal laser, photodynamic therapy (PDT), and surgery can be applied [2]. There are two methods for surgical draining SRF: internal and external approach. Internal drainage may lead to retinotomy-associated rhegmatogenous retinal detachment (RD) [3]. Pars plana vitrectomy (PPV) with external drainage does not need retinotomy, allowing laser photocoagulation with an improved view using perfluorocarbon liquid (PFCL) and immediate retinal reattachment [4]. We report a case of bCSC treated with external drainage and vitrectomy in which the retina was reattached and maintained without recurrence for more than 1.5 years. Informed consent was obtained from the patient for publication of this case report and relevant images. A 51-year-old male patient presented with blurred vision in his right eye that started 5 days ago. Uncorrected visual acuity was 20 / 20, and intraocular pressure was normal in both eyes. Anterior segment was unremarkable. Fundus showed inferior bullous RD and no breaks in the right eye (Fig. 1A). Fundus was normal in the left eye. Perifoveal PEDs were found in the right eye (Fig. 1B). SRF increased the day after admission (Fig. 1C, 1D). Fluorescein angiography showed multiple perifoveal leaking points, a main inferonasal leaking point, and consequent pooling to the subretinal space (Fig. 1E, 1F). Optical coherence tomography (OCT) showed RPE tear at the site corresponding to the main leaking point (Fig. 1G). Exudative RD secondary to CSC (i.e., bCSC) was diagnosed and laser photocoagulation at leaking points was performed. On the 3rd day of admission, best-corrected visual acuity (BCVA) was 20 / 40, fundus showed shifting of SRF after sleeping on one side (Fig. 1H). Indocyanine green angiography shows hyper-permeable and dilated choroidal vessels (Fig. 1I). SRF decreased in OCT (Fig. 1J). He was discharged on the 5th day of admission. However, SRF increased significantly, and BCVA was 20 / 67 at outpatient visit at 5 days after discharge. We decided to transfer him for PDT. The next day, he was transferred to another hospital. BCVA decreased to finger count. Exudative RD was extended and prominent (Fig. 1K, 1L). Therefore, PDT was considered ineffective. After waiting 1 week, RD was further extended, and surgery was performed by SJW (Fig. 1M-1O). External drainage, PPV with perfluorocarbon liquid, endolaser, and intravitreal sulfur hexafluoride 18% gas injection were performed (Supplementary Video 1). Three months after surgery, BCVA was 20 / 40 and fundus showed flat retina and laser markings at nasal midperiphery (Fig. 1P, 1Q). One year and 8 months after surgery, BCVA was 20 / 29 and fundus was flat (Fig. 1R, 1S). To the best of our knowledge, this is the first report of bCSC successfully treated with external drainage and vitrectomy in Korea. Kang et al. [5] presented bilateral bCSC treated with internal drainage and vitrectomy. Their patient was initially treated with corticosteroid under diagnosis of Vogt–Koyanagi–Harada. Despite focal laser, exudative RD extended to fovea. External drainage, intravitreal gas injection, scleral buckling, and focal laser were applied. After 2 months, internal drainage, PPV, intravitreal gas injection, and focal laser were performed for recurrent RD [5]. In contrast, in our case, retina was attached and remained without recurrence during about 1.5 years after external drainage. In the study by Kang et al. [5], initial surKorean J Ophthalmol 2022;36(6):575-577 https://doi.org/10.3341/kjo.2022.0099

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


