{"title":"早期经验性Anidulafungin降低危重患者侵袭性念珠菌病的患病率:一项病例对照研究。","authors":"Md Jahidul Hasan, Sharmind Neelotpol, Raihan Rabbani","doi":"10.2478/jccm-2022-0006","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Invasive candidiasis (IC) in critically ill patients is a serious infection with high rate of mortality. As an empirical therapy, like antibiotics, the use of antifungals is not common in intensive care units (ICUs) worldwide. The empirical use of echinocandins including anidulafungin is a recent trend.</p><p><strong>Aim of the study: </strong>The objective of this study was to assess the impact of empirical anidulafungin in the development of invasive candidiasis in critically ill patients in ICU.</p><p><strong>Methods: </strong>This retrospective case-control study was conducted on 149 patients with sepsis with/without septic shock and bacterial pneumonia. All the patients were divided into two groups. The 'control group' termed as 'NEAT group' received no empirical anidulafungin therapy and the 'treated group' termed as 'EAT group' received empirical anidulafungin therapy in early hospitalization hours.</p><p><strong>Results: </strong>Seventy-two and 77 patients were divided into the control and the treated group, respectively. Patients in EAT group showed less incidences of IC (5.19%) than that of the NEAT group (29.17%) (p = 0.001). Here, the relative risk (RR) was 0.175 (95% CI, 0.064-0.493) and the risk difference (RD) rate was 24% (95% CI, 12.36%-35.58%). The 30-day all-cause mortality rate in NEAT group was higher (19.44%) than that of in EAT group (10.39%) (p = 0.04). Within the first 10-ICU-day, patients in the EAT group left ICU in higher rate (62.34%) than that in the NEAT group (54.17%).</p><p><strong>Conclusion: </strong>Early empirical anidulafungin within 6 h of ICU admission reduced the risk of invasive candidiasis, 30-day all-cause mortality rate and increased ICU leaving rate within 10-day of ICU admission in critically ill patients.</p>","PeriodicalId":73696,"journal":{"name":"","volume":"8 2","pages":"89-99"},"PeriodicalIF":0.0,"publicationDate":"2022-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9097641/pdf/","citationCount":"0","resultStr":"{\"title\":\"Early Empirical Anidulafungin Reduces the Prevalence of Invasive Candidiasis in Critically Ill Patients: A Case-control Study.\",\"authors\":\"Md Jahidul Hasan, Sharmind Neelotpol, Raihan Rabbani\",\"doi\":\"10.2478/jccm-2022-0006\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Invasive candidiasis (IC) in critically ill patients is a serious infection with high rate of mortality. As an empirical therapy, like antibiotics, the use of antifungals is not common in intensive care units (ICUs) worldwide. The empirical use of echinocandins including anidulafungin is a recent trend.</p><p><strong>Aim of the study: </strong>The objective of this study was to assess the impact of empirical anidulafungin in the development of invasive candidiasis in critically ill patients in ICU.</p><p><strong>Methods: </strong>This retrospective case-control study was conducted on 149 patients with sepsis with/without septic shock and bacterial pneumonia. All the patients were divided into two groups. The 'control group' termed as 'NEAT group' received no empirical anidulafungin therapy and the 'treated group' termed as 'EAT group' received empirical anidulafungin therapy in early hospitalization hours.</p><p><strong>Results: </strong>Seventy-two and 77 patients were divided into the control and the treated group, respectively. Patients in EAT group showed less incidences of IC (5.19%) than that of the NEAT group (29.17%) (p = 0.001). Here, the relative risk (RR) was 0.175 (95% CI, 0.064-0.493) and the risk difference (RD) rate was 24% (95% CI, 12.36%-35.58%). The 30-day all-cause mortality rate in NEAT group was higher (19.44%) than that of in EAT group (10.39%) (p = 0.04). Within the first 10-ICU-day, patients in the EAT group left ICU in higher rate (62.34%) than that in the NEAT group (54.17%).</p><p><strong>Conclusion: </strong>Early empirical anidulafungin within 6 h of ICU admission reduced the risk of invasive candidiasis, 30-day all-cause mortality rate and increased ICU leaving rate within 10-day of ICU admission in critically ill patients.</p>\",\"PeriodicalId\":73696,\"journal\":{\"name\":\"\",\"volume\":\"8 2\",\"pages\":\"89-99\"},\"PeriodicalIF\":0.0,\"publicationDate\":\"2022-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9097641/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2478/jccm-2022-0006\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2478/jccm-2022-0006","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Early Empirical Anidulafungin Reduces the Prevalence of Invasive Candidiasis in Critically Ill Patients: A Case-control Study.
Introduction: Invasive candidiasis (IC) in critically ill patients is a serious infection with high rate of mortality. As an empirical therapy, like antibiotics, the use of antifungals is not common in intensive care units (ICUs) worldwide. The empirical use of echinocandins including anidulafungin is a recent trend.
Aim of the study: The objective of this study was to assess the impact of empirical anidulafungin in the development of invasive candidiasis in critically ill patients in ICU.
Methods: This retrospective case-control study was conducted on 149 patients with sepsis with/without septic shock and bacterial pneumonia. All the patients were divided into two groups. The 'control group' termed as 'NEAT group' received no empirical anidulafungin therapy and the 'treated group' termed as 'EAT group' received empirical anidulafungin therapy in early hospitalization hours.
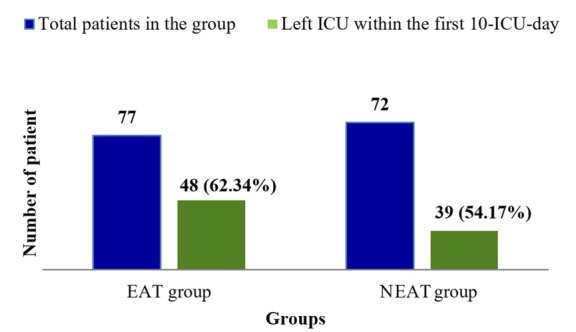
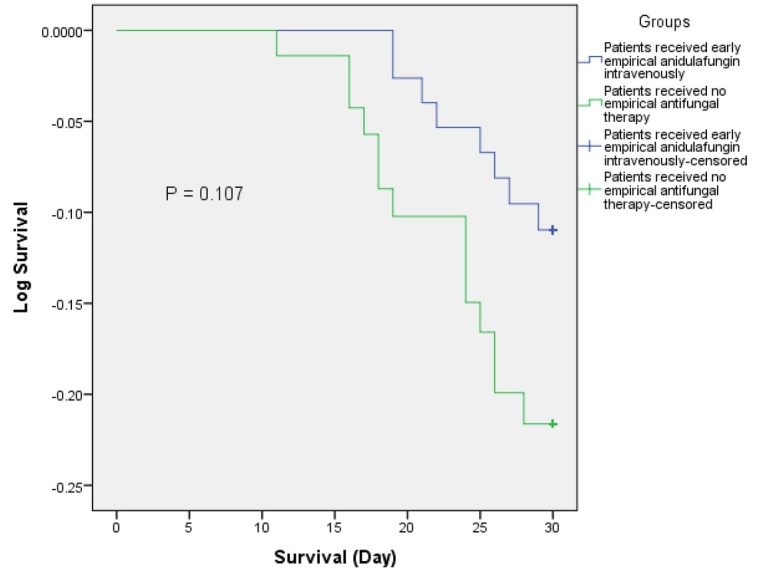
Results: Seventy-two and 77 patients were divided into the control and the treated group, respectively. Patients in EAT group showed less incidences of IC (5.19%) than that of the NEAT group (29.17%) (p = 0.001). Here, the relative risk (RR) was 0.175 (95% CI, 0.064-0.493) and the risk difference (RD) rate was 24% (95% CI, 12.36%-35.58%). The 30-day all-cause mortality rate in NEAT group was higher (19.44%) than that of in EAT group (10.39%) (p = 0.04). Within the first 10-ICU-day, patients in the EAT group left ICU in higher rate (62.34%) than that in the NEAT group (54.17%).
Conclusion: Early empirical anidulafungin within 6 h of ICU admission reduced the risk of invasive candidiasis, 30-day all-cause mortality rate and increased ICU leaving rate within 10-day of ICU admission in critically ill patients.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


