Dario Amore, Dino Casazza, Marco Rispoli, Cristiano Cesaro, Emanuele Muto, Pasquale Imitazione, Carlo Curcio
{"title":"获得性良性气管食管瘘:一种可选择的气管整形技术。","authors":"Dario Amore, Dino Casazza, Marco Rispoli, Cristiano Cesaro, Emanuele Muto, Pasquale Imitazione, Carlo Curcio","doi":"10.5761/atcs.nm.22-00077","DOIUrl":null,"url":null,"abstract":"<p><p>We present a case of surgical management of a tracheoesophageal fistula (TEF) following prolonged intubation. After transverse tracheal division and retraction of the distal stump, direct closure of the esophageal defect and repair of the membranous tracheal defect using a synthetic bioabsorbable patch were performed, followed by interposition of muscle flap between the suture lines and tracheal reconstruction. Large TEFs, without tracheal stenosis or circumferential airway defect, associated with marked peritracheal inflammation, may be treated with this alternative tracheoplastic technique in patients deemed not suitable for tracheal resection and anastomosis.</p>","PeriodicalId":8037,"journal":{"name":"Annals of Thoracic and Cardiovascular Surgery","volume":"28 6","pages":"377-380"},"PeriodicalIF":1.3000,"publicationDate":"2022-12-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ed/fe/atcs-28-377.PMC9763712.pdf","citationCount":"2","resultStr":"{\"title\":\"Acquired Benign Tracheoesophageal Fistula: An Alternative Tracheoplastic Technique.\",\"authors\":\"Dario Amore, Dino Casazza, Marco Rispoli, Cristiano Cesaro, Emanuele Muto, Pasquale Imitazione, Carlo Curcio\",\"doi\":\"10.5761/atcs.nm.22-00077\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>We present a case of surgical management of a tracheoesophageal fistula (TEF) following prolonged intubation. After transverse tracheal division and retraction of the distal stump, direct closure of the esophageal defect and repair of the membranous tracheal defect using a synthetic bioabsorbable patch were performed, followed by interposition of muscle flap between the suture lines and tracheal reconstruction. Large TEFs, without tracheal stenosis or circumferential airway defect, associated with marked peritracheal inflammation, may be treated with this alternative tracheoplastic technique in patients deemed not suitable for tracheal resection and anastomosis.</p>\",\"PeriodicalId\":8037,\"journal\":{\"name\":\"Annals of Thoracic and Cardiovascular Surgery\",\"volume\":\"28 6\",\"pages\":\"377-380\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2022-12-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ed/fe/atcs-28-377.PMC9763712.pdf\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Thoracic and Cardiovascular Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.5761/atcs.nm.22-00077\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Thoracic and Cardiovascular Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5761/atcs.nm.22-00077","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Acquired Benign Tracheoesophageal Fistula: An Alternative Tracheoplastic Technique.
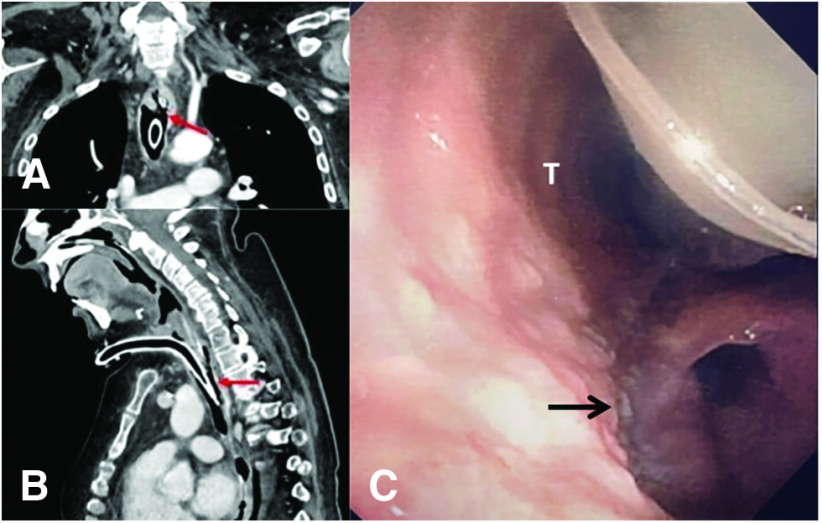
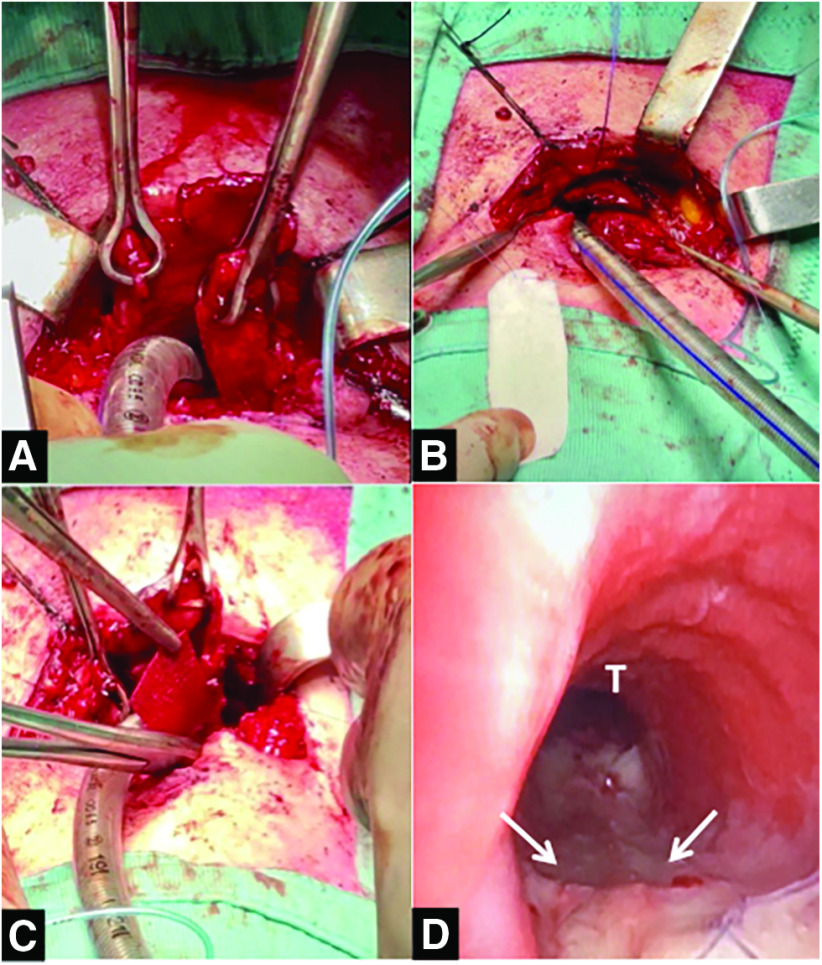
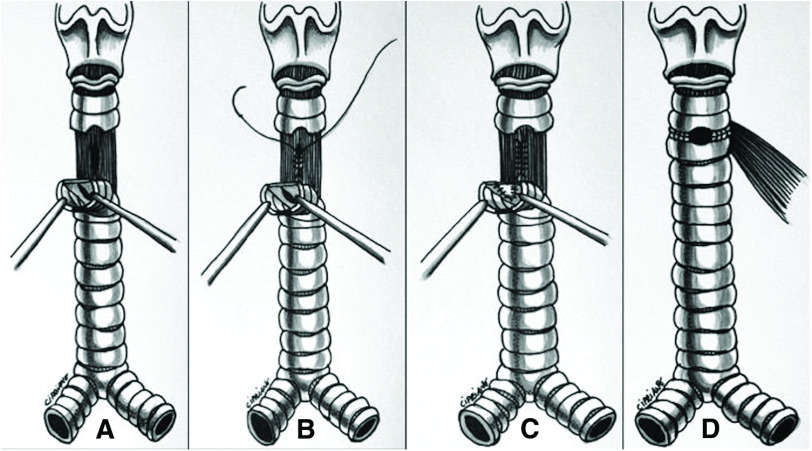
We present a case of surgical management of a tracheoesophageal fistula (TEF) following prolonged intubation. After transverse tracheal division and retraction of the distal stump, direct closure of the esophageal defect and repair of the membranous tracheal defect using a synthetic bioabsorbable patch were performed, followed by interposition of muscle flap between the suture lines and tracheal reconstruction. Large TEFs, without tracheal stenosis or circumferential airway defect, associated with marked peritracheal inflammation, may be treated with this alternative tracheoplastic technique in patients deemed not suitable for tracheal resection and anastomosis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


