Asad E Patanwala, Danijela Spremo, Minji Jeon, Yann Thoma, Jan-Willem C Alffenaar, Sophie Stocker
{"title":"贝叶斯万古霉素模型之间的差异会影响危重患者的临床决策。","authors":"Asad E Patanwala, Danijela Spremo, Minji Jeon, Yann Thoma, Jan-Willem C Alffenaar, Sophie Stocker","doi":"10.1155/2022/7011376","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>To assess the agreement in 24-hour area under the curve (AUC<sub>24</sub>) value estimates between commonly used vancomycin population pharmacokinetic models in the critically ill.</p><p><strong>Materials and methods: </strong>Adults admitted to intensive care who received intravenous vancomycin and had a serum vancomycin concentration available were included. AUC<sub>24</sub> values were determined using Tucuxi (revision cd7bd7a8) for dosing intervals with a vancomycin concentration using three models (Goti 2018, Colin 2019, and Thomson 2009) previously evaluated in the critically ill. AUC<sub>24</sub> values were categorized as subtherapeutic (<400 mg·h/L), therapeutic (400-600 mg·h/L), or toxic (>600 mg·h/L), assuming a minimum inhibitory concentration of 1 mg/L. AUC<sub>24</sub> value categorization was compared across the three models and reported as percent agreement.</p><p><strong>Results: </strong>Overall, 466 AUC<sub>24</sub> values were estimated in 188 patients. Overall, 52%, 42%, and 47% of the AUC<sub>24</sub> values were therapeutic for the Goti, Colin, and Thomson models, respectively. The agreement of AUC<sub>24</sub> values between all three models was 48% (223/466), Goti-Colin 59% (193/466), Goti-Thomson 68% (318/466), and Colin-Thomson 67% (314/466).</p><p><strong>Conclusion: </strong>In critically ill patients, vancomycin AUC<sub>24</sub> values obtained from different pharmacokinetic models are often discordant, potentially contributing to differences in dosing decisions. This highlights the importance of selecting the optimal model.</p>","PeriodicalId":46583,"journal":{"name":"Critical Care Research and Practice","volume":"2022 ","pages":"7011376"},"PeriodicalIF":1.8000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9767744/pdf/","citationCount":"0","resultStr":"{\"title\":\"Discrepancies Between Bayesian Vancomycin Models Can Affect Clinical Decisions in the Critically Ill.\",\"authors\":\"Asad E Patanwala, Danijela Spremo, Minji Jeon, Yann Thoma, Jan-Willem C Alffenaar, Sophie Stocker\",\"doi\":\"10.1155/2022/7011376\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>To assess the agreement in 24-hour area under the curve (AUC<sub>24</sub>) value estimates between commonly used vancomycin population pharmacokinetic models in the critically ill.</p><p><strong>Materials and methods: </strong>Adults admitted to intensive care who received intravenous vancomycin and had a serum vancomycin concentration available were included. AUC<sub>24</sub> values were determined using Tucuxi (revision cd7bd7a8) for dosing intervals with a vancomycin concentration using three models (Goti 2018, Colin 2019, and Thomson 2009) previously evaluated in the critically ill. AUC<sub>24</sub> values were categorized as subtherapeutic (<400 mg·h/L), therapeutic (400-600 mg·h/L), or toxic (>600 mg·h/L), assuming a minimum inhibitory concentration of 1 mg/L. AUC<sub>24</sub> value categorization was compared across the three models and reported as percent agreement.</p><p><strong>Results: </strong>Overall, 466 AUC<sub>24</sub> values were estimated in 188 patients. Overall, 52%, 42%, and 47% of the AUC<sub>24</sub> values were therapeutic for the Goti, Colin, and Thomson models, respectively. The agreement of AUC<sub>24</sub> values between all three models was 48% (223/466), Goti-Colin 59% (193/466), Goti-Thomson 68% (318/466), and Colin-Thomson 67% (314/466).</p><p><strong>Conclusion: </strong>In critically ill patients, vancomycin AUC<sub>24</sub> values obtained from different pharmacokinetic models are often discordant, potentially contributing to differences in dosing decisions. This highlights the importance of selecting the optimal model.</p>\",\"PeriodicalId\":46583,\"journal\":{\"name\":\"Critical Care Research and Practice\",\"volume\":\"2022 \",\"pages\":\"7011376\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2022-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9767744/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical Care Research and Practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2022/7011376\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Care Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2022/7011376","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
Discrepancies Between Bayesian Vancomycin Models Can Affect Clinical Decisions in the Critically Ill.
Purpose: To assess the agreement in 24-hour area under the curve (AUC24) value estimates between commonly used vancomycin population pharmacokinetic models in the critically ill.
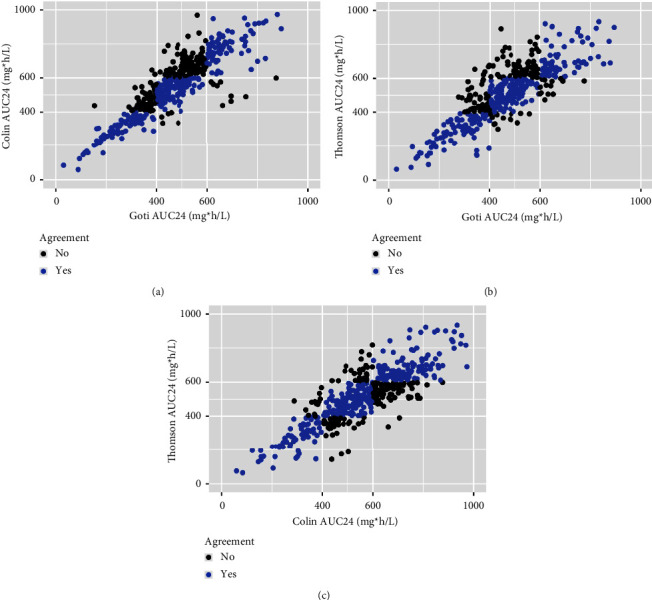
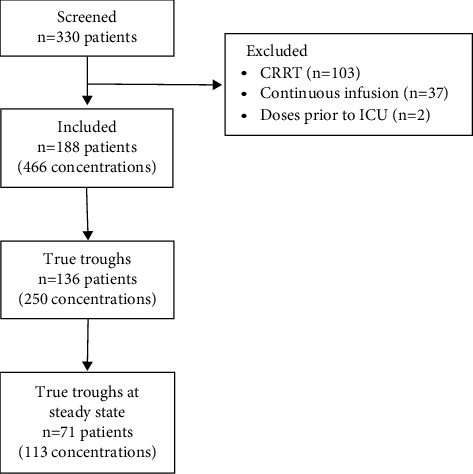
Materials and methods: Adults admitted to intensive care who received intravenous vancomycin and had a serum vancomycin concentration available were included. AUC24 values were determined using Tucuxi (revision cd7bd7a8) for dosing intervals with a vancomycin concentration using three models (Goti 2018, Colin 2019, and Thomson 2009) previously evaluated in the critically ill. AUC24 values were categorized as subtherapeutic (<400 mg·h/L), therapeutic (400-600 mg·h/L), or toxic (>600 mg·h/L), assuming a minimum inhibitory concentration of 1 mg/L. AUC24 value categorization was compared across the three models and reported as percent agreement.
Results: Overall, 466 AUC24 values were estimated in 188 patients. Overall, 52%, 42%, and 47% of the AUC24 values were therapeutic for the Goti, Colin, and Thomson models, respectively. The agreement of AUC24 values between all three models was 48% (223/466), Goti-Colin 59% (193/466), Goti-Thomson 68% (318/466), and Colin-Thomson 67% (314/466).
Conclusion: In critically ill patients, vancomycin AUC24 values obtained from different pharmacokinetic models are often discordant, potentially contributing to differences in dosing decisions. This highlights the importance of selecting the optimal model.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


