Jens Johansson Ramgren MD , Shahab Nozohoor MD, PhD , Igor Zindovic MD, PhD , Ronny Gustafsson MD, PhD , Nina Hakacova MD, PhD , Johan Sjögren MD, PhD
{"title":"房室间隔缺损修复后再手术:25年以上单一中心经验","authors":"Jens Johansson Ramgren MD , Shahab Nozohoor MD, PhD , Igor Zindovic MD, PhD , Ronny Gustafsson MD, PhD , Nina Hakacova MD, PhD , Johan Sjögren MD, PhD","doi":"10.1053/j.semtcvs.2022.06.008","DOIUrl":null,"url":null,"abstract":"<div><p><span><span>Our aim was to evaluate the total burden of reoperations<span> after previous repair for atrioventricular septal defects<span>, including long-term survival and identify risk factors for reoperation. All patients with surgical correction for atrioventricular septal defect (AVSD) 1993- 2020 underwent a follow-up in October 2020. Clinical data were obtained by retrospective review and evaluated with Kaplan-Meier and competing risk analysis. Of 477 patients who underwent initial repair, 53 patients (11.1%) underwent a total of 82 reoperations. The perioperative mortality at reoperation was 3.8% (2/53). There were no late deaths (0/51) during follow-up. </span></span></span>In patients<span> requiring reoperation for left atrioventricular valve regurgitation, a re-repair was performed in 90% (26/29) at first attempt. Estimated overall survival was 96.2 ± 2.6% (95% CI 91.2-100) in the Any reoperation group and 96.7 ± 0.9% (95% CI 94.9-98.5) in the No reoperation group at 20 years (</span></span><em>P</em> = 0.80). The cumulative incidence function of Any reoperation (with death as competing risk) was 13.0% (95% CI 9.4-16.5) at 20 years. Independent risk factors for Any reoperation included severe mitral regurgitation after primary repair (HR 40.7; 95% CI 14.9-111; <em>P</em><span> < 0.001). The risk of perioperative mortality in AVSD patients undergoing reoperation was low in the present study. Long-term survival was very good and not significantly different when compared to patients who did not need reoperation. Re-repair for left atrioventricular valve regurgitation was possible in most cases and showed long-term durability. Our data suggest that reoperations after primary repair of AVSD have very good long-term outcomes when performed at a high-volume pediatric cardiac surgery center.</span></p></div>","PeriodicalId":48592,"journal":{"name":"Seminars in Thoracic and Cardiovascular Surgery","volume":"35 3","pages":"Pages 530-538"},"PeriodicalIF":2.6000,"publicationDate":"2023-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"1","resultStr":"{\"title\":\"Reoperations After Repair for Atrioventricular Septal Defects: >25 Years Experience at a Single Center\",\"authors\":\"Jens Johansson Ramgren MD , Shahab Nozohoor MD, PhD , Igor Zindovic MD, PhD , Ronny Gustafsson MD, PhD , Nina Hakacova MD, PhD , Johan Sjögren MD, PhD\",\"doi\":\"10.1053/j.semtcvs.2022.06.008\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><p><span><span>Our aim was to evaluate the total burden of reoperations<span> after previous repair for atrioventricular septal defects<span>, including long-term survival and identify risk factors for reoperation. All patients with surgical correction for atrioventricular septal defect (AVSD) 1993- 2020 underwent a follow-up in October 2020. Clinical data were obtained by retrospective review and evaluated with Kaplan-Meier and competing risk analysis. Of 477 patients who underwent initial repair, 53 patients (11.1%) underwent a total of 82 reoperations. The perioperative mortality at reoperation was 3.8% (2/53). There were no late deaths (0/51) during follow-up. </span></span></span>In patients<span> requiring reoperation for left atrioventricular valve regurgitation, a re-repair was performed in 90% (26/29) at first attempt. Estimated overall survival was 96.2 ± 2.6% (95% CI 91.2-100) in the Any reoperation group and 96.7 ± 0.9% (95% CI 94.9-98.5) in the No reoperation group at 20 years (</span></span><em>P</em> = 0.80). The cumulative incidence function of Any reoperation (with death as competing risk) was 13.0% (95% CI 9.4-16.5) at 20 years. Independent risk factors for Any reoperation included severe mitral regurgitation after primary repair (HR 40.7; 95% CI 14.9-111; <em>P</em><span> < 0.001). The risk of perioperative mortality in AVSD patients undergoing reoperation was low in the present study. Long-term survival was very good and not significantly different when compared to patients who did not need reoperation. Re-repair for left atrioventricular valve regurgitation was possible in most cases and showed long-term durability. Our data suggest that reoperations after primary repair of AVSD have very good long-term outcomes when performed at a high-volume pediatric cardiac surgery center.</span></p></div>\",\"PeriodicalId\":48592,\"journal\":{\"name\":\"Seminars in Thoracic and Cardiovascular Surgery\",\"volume\":\"35 3\",\"pages\":\"Pages 530-538\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2023-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Seminars in Thoracic and Cardiovascular Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S104306792200140X\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Seminars in Thoracic and Cardiovascular Surgery","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S104306792200140X","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
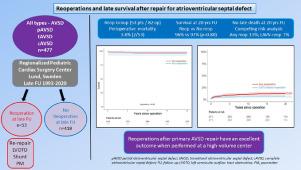
Reoperations After Repair for Atrioventricular Septal Defects: >25 Years Experience at a Single Center
Our aim was to evaluate the total burden of reoperations after previous repair for atrioventricular septal defects, including long-term survival and identify risk factors for reoperation. All patients with surgical correction for atrioventricular septal defect (AVSD) 1993- 2020 underwent a follow-up in October 2020. Clinical data were obtained by retrospective review and evaluated with Kaplan-Meier and competing risk analysis. Of 477 patients who underwent initial repair, 53 patients (11.1%) underwent a total of 82 reoperations. The perioperative mortality at reoperation was 3.8% (2/53). There were no late deaths (0/51) during follow-up. In patients requiring reoperation for left atrioventricular valve regurgitation, a re-repair was performed in 90% (26/29) at first attempt. Estimated overall survival was 96.2 ± 2.6% (95% CI 91.2-100) in the Any reoperation group and 96.7 ± 0.9% (95% CI 94.9-98.5) in the No reoperation group at 20 years (P = 0.80). The cumulative incidence function of Any reoperation (with death as competing risk) was 13.0% (95% CI 9.4-16.5) at 20 years. Independent risk factors for Any reoperation included severe mitral regurgitation after primary repair (HR 40.7; 95% CI 14.9-111; P < 0.001). The risk of perioperative mortality in AVSD patients undergoing reoperation was low in the present study. Long-term survival was very good and not significantly different when compared to patients who did not need reoperation. Re-repair for left atrioventricular valve regurgitation was possible in most cases and showed long-term durability. Our data suggest that reoperations after primary repair of AVSD have very good long-term outcomes when performed at a high-volume pediatric cardiac surgery center.
期刊介绍:
Seminars in Thoracic and Cardiovascular Surgery is devoted to providing a forum for cardiothoracic surgeons to disseminate and discuss important new information and to gain insight into unresolved areas of question in the specialty. Each issue presents readers with a selection of original peer-reviewed articles accompanied by editorial commentary from specialists in the field. In addition, readers are offered valuable invited articles: State of Views editorials and Current Readings highlighting the latest contributions on central or controversial issues. Another prized feature is expert roundtable discussions in which experts debate critical questions for cardiothoracic treatment and care. Seminars is an invitation-only publication that receives original submissions transferred ONLY from its sister publication, The Journal of Thoracic and Cardiovascular Surgery. As we continue to expand the reach of the Journal, we will explore the possibility of accepting unsolicited manuscripts in the future.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


