Natalie E Sheils, Megan S Jarvis, Lauren R Bangerter, David A Asch, Callahan N Clark
{"title":"使用大型行政索赔数据库的美国参保人群中2型糖尿病缓解的真实患病率。","authors":"Natalie E Sheils, Megan S Jarvis, Lauren R Bangerter, David A Asch, Callahan N Clark","doi":"10.2337/ds22-0042","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>A 2021 international consensus statement defined type 2 diabetes remission as A1C <6.5% measured at least 3 months after cessation of glucose-lowering therapy. We aimed to investigate whether retrospective claims-based data can assess remission based on this definition, whether three increasingly strict alternative definitions affect the prevalence of remission and characteristics of remission cohorts, and how cohorts with and without sufficient data to assess for remission differ.</p><p><strong>Research design and methods: </strong>We used de-identified administrative claims from commercially insured and Medicare Advantage members, enriched with laboratory values, to assess diabetes remission. We used alternative glycemic, temporal, and pharmacologic criteria to assess the sensitivity of remission definitions to changes in claims-based logic.</p><p><strong>Results: </strong>Among 524,076 adults with type 2 diabetes, 185,285 (35.4%) had insufficient additional laboratory and/or enrollment data to assess for remission. While more likely to be younger, these individuals had similar initial A1C values and geographical distribution as the 338,791 (64.6%) assessed for remission. Of those assessed for remission, 10,694 (3.2%) met the 2021 consensus statement definition. The proportion of individuals meeting the three alternative definitions ranged from 0.8 to 2.3%. Across all criteria, those meeting the remission definition were more likely to be female, had a lower initially observed A1C, and had a higher prevalence of bariatric surgery.</p><p><strong>Conclusion: </strong>This study demonstrates the feasibility of laboratory-value enriched claims-based assessments of type 2 diabetes remission. Establishing stable claims-based markers of remission can enable population assessments of diabetes remission and evaluate the association between remission and clinical outcomes.</p>","PeriodicalId":72797,"journal":{"name":"","volume":"36 3","pages":"211-218"},"PeriodicalIF":0.0,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10425229/pdf/","citationCount":"0","resultStr":"{\"title\":\"Real-World Prevalence of Type 2 Diabetes Remission in a U.S. Insured Population Using a Large Administrative Claims Database.\",\"authors\":\"Natalie E Sheils, Megan S Jarvis, Lauren R Bangerter, David A Asch, Callahan N Clark\",\"doi\":\"10.2337/ds22-0042\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>A 2021 international consensus statement defined type 2 diabetes remission as A1C <6.5% measured at least 3 months after cessation of glucose-lowering therapy. We aimed to investigate whether retrospective claims-based data can assess remission based on this definition, whether three increasingly strict alternative definitions affect the prevalence of remission and characteristics of remission cohorts, and how cohorts with and without sufficient data to assess for remission differ.</p><p><strong>Research design and methods: </strong>We used de-identified administrative claims from commercially insured and Medicare Advantage members, enriched with laboratory values, to assess diabetes remission. We used alternative glycemic, temporal, and pharmacologic criteria to assess the sensitivity of remission definitions to changes in claims-based logic.</p><p><strong>Results: </strong>Among 524,076 adults with type 2 diabetes, 185,285 (35.4%) had insufficient additional laboratory and/or enrollment data to assess for remission. While more likely to be younger, these individuals had similar initial A1C values and geographical distribution as the 338,791 (64.6%) assessed for remission. Of those assessed for remission, 10,694 (3.2%) met the 2021 consensus statement definition. The proportion of individuals meeting the three alternative definitions ranged from 0.8 to 2.3%. Across all criteria, those meeting the remission definition were more likely to be female, had a lower initially observed A1C, and had a higher prevalence of bariatric surgery.</p><p><strong>Conclusion: </strong>This study demonstrates the feasibility of laboratory-value enriched claims-based assessments of type 2 diabetes remission. Establishing stable claims-based markers of remission can enable population assessments of diabetes remission and evaluate the association between remission and clinical outcomes.</p>\",\"PeriodicalId\":72797,\"journal\":{\"name\":\"\",\"volume\":\"36 3\",\"pages\":\"211-218\"},\"PeriodicalIF\":0.0,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10425229/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2337/ds22-0042\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2337/ds22-0042","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Real-World Prevalence of Type 2 Diabetes Remission in a U.S. Insured Population Using a Large Administrative Claims Database.
Objective: A 2021 international consensus statement defined type 2 diabetes remission as A1C <6.5% measured at least 3 months after cessation of glucose-lowering therapy. We aimed to investigate whether retrospective claims-based data can assess remission based on this definition, whether three increasingly strict alternative definitions affect the prevalence of remission and characteristics of remission cohorts, and how cohorts with and without sufficient data to assess for remission differ.
Research design and methods: We used de-identified administrative claims from commercially insured and Medicare Advantage members, enriched with laboratory values, to assess diabetes remission. We used alternative glycemic, temporal, and pharmacologic criteria to assess the sensitivity of remission definitions to changes in claims-based logic.
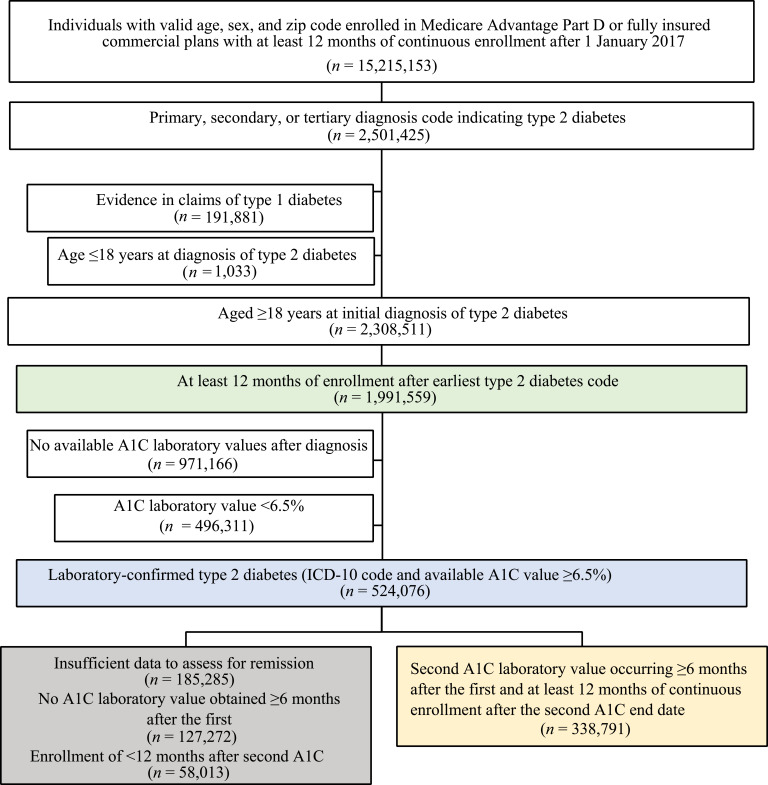
Results: Among 524,076 adults with type 2 diabetes, 185,285 (35.4%) had insufficient additional laboratory and/or enrollment data to assess for remission. While more likely to be younger, these individuals had similar initial A1C values and geographical distribution as the 338,791 (64.6%) assessed for remission. Of those assessed for remission, 10,694 (3.2%) met the 2021 consensus statement definition. The proportion of individuals meeting the three alternative definitions ranged from 0.8 to 2.3%. Across all criteria, those meeting the remission definition were more likely to be female, had a lower initially observed A1C, and had a higher prevalence of bariatric surgery.
Conclusion: This study demonstrates the feasibility of laboratory-value enriched claims-based assessments of type 2 diabetes remission. Establishing stable claims-based markers of remission can enable population assessments of diabetes remission and evaluate the association between remission and clinical outcomes.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


