Ariel Wimpfheimer, Charles Weissman, Shai Fein, Yehuda Ginosar
{"title":"当政策遇到现实:新的18小时随叫随到轮班政策和以色列麻醉劳动力危机。","authors":"Ariel Wimpfheimer, Charles Weissman, Shai Fein, Yehuda Ginosar","doi":"10.1186/s13584-023-00556-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The Israeli physician workforce faces multiple challenges. These include planned policies reducing physician on-call from 26 to 18 h and, from 2026, allowing only graduates of Ministry of Health approved foreign medical schools to take the Israeli licensing examination and an ongoing physician shortage (2019: Israel had 3.19 physicians/1000 persons vs. OECD average of 3.49 physicians/1000 persons). This study examines the potential impact of these planned policies on the Israeli anesthesiology workforce.</p><p><strong>Methods: </strong>Surveys conducted among 34 public and private Israeli hospital anesthesiology department chairs collected data on their department's number of weekday on-call anesthesiologists and current shortage of anesthesiologists. A subsequent survey collected data on each anesthesiologist in the workforce, including the country where they studied medicine.</p><p><strong>Results: </strong>Each weekday night there were 114 on-call anesthesiologists; 72 residents and 42 attendings. Using productive work coefficients, this translates to 104 resident and 51 attending anesthesiologists. Furthermore, 21 departments had existing anesthesia workforce shortages totaling 110 anesthesiologists. There were 873 anesthesiologists from non-OECD countries whose medical schools are not accredited by the World Federation for Medical Education, of whom 332 were residents (61.9% of residents). Only 20.1% of anesthesiology residents were Israeli medical school graduates.</p><p><strong>Conclusions: </strong>Descriptive survey data assessed the immediate and long-term consequences for the healthcare system and anesthesiology workforce of two new Health Ministry policies. Implementing the 18-h policy will immediately remove from the daytime workforce 155 anesthesiologists and who will be unavailable to staff elective surgery operating rooms. This will compound the current national shortage of 110 anesthesiologists. It is unclear how to replace this shortfall since there are no surplus Israeli physicians and very few Israeli graduates choose anesthesiology as a specialty. This situation will be exacerbated after 2026 when graduates of certain foreign medical schools will be unable to enter the medical workforce, further reducing the pool of potential anesthesiology residents. Both policies were promulgated without adequate operational and budgetary planning or fiscal or workforce resources; implementation of the 18-h on-call policy has already been postponed. Therefore, new or updated policies must be accompanied by specific operational plans, budgetary allocations and funds for additional workforce.</p>","PeriodicalId":46694,"journal":{"name":"Israel Journal of Health Policy Research","volume":"12 1","pages":"8"},"PeriodicalIF":3.5000,"publicationDate":"2023-03-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9977473/pdf/","citationCount":"1","resultStr":"{\"title\":\"When policy meets reality: the new 18-hour on-call shift policy and the Israeli anesthesia workforce crisis.\",\"authors\":\"Ariel Wimpfheimer, Charles Weissman, Shai Fein, Yehuda Ginosar\",\"doi\":\"10.1186/s13584-023-00556-x\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The Israeli physician workforce faces multiple challenges. These include planned policies reducing physician on-call from 26 to 18 h and, from 2026, allowing only graduates of Ministry of Health approved foreign medical schools to take the Israeli licensing examination and an ongoing physician shortage (2019: Israel had 3.19 physicians/1000 persons vs. OECD average of 3.49 physicians/1000 persons). This study examines the potential impact of these planned policies on the Israeli anesthesiology workforce.</p><p><strong>Methods: </strong>Surveys conducted among 34 public and private Israeli hospital anesthesiology department chairs collected data on their department's number of weekday on-call anesthesiologists and current shortage of anesthesiologists. A subsequent survey collected data on each anesthesiologist in the workforce, including the country where they studied medicine.</p><p><strong>Results: </strong>Each weekday night there were 114 on-call anesthesiologists; 72 residents and 42 attendings. Using productive work coefficients, this translates to 104 resident and 51 attending anesthesiologists. Furthermore, 21 departments had existing anesthesia workforce shortages totaling 110 anesthesiologists. There were 873 anesthesiologists from non-OECD countries whose medical schools are not accredited by the World Federation for Medical Education, of whom 332 were residents (61.9% of residents). Only 20.1% of anesthesiology residents were Israeli medical school graduates.</p><p><strong>Conclusions: </strong>Descriptive survey data assessed the immediate and long-term consequences for the healthcare system and anesthesiology workforce of two new Health Ministry policies. Implementing the 18-h policy will immediately remove from the daytime workforce 155 anesthesiologists and who will be unavailable to staff elective surgery operating rooms. This will compound the current national shortage of 110 anesthesiologists. It is unclear how to replace this shortfall since there are no surplus Israeli physicians and very few Israeli graduates choose anesthesiology as a specialty. This situation will be exacerbated after 2026 when graduates of certain foreign medical schools will be unable to enter the medical workforce, further reducing the pool of potential anesthesiology residents. Both policies were promulgated without adequate operational and budgetary planning or fiscal or workforce resources; implementation of the 18-h on-call policy has already been postponed. Therefore, new or updated policies must be accompanied by specific operational plans, budgetary allocations and funds for additional workforce.</p>\",\"PeriodicalId\":46694,\"journal\":{\"name\":\"Israel Journal of Health Policy Research\",\"volume\":\"12 1\",\"pages\":\"8\"},\"PeriodicalIF\":3.5000,\"publicationDate\":\"2023-03-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9977473/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Israel Journal of Health Policy Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13584-023-00556-x\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"HEALTH POLICY & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Israel Journal of Health Policy Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13584-023-00556-x","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEALTH POLICY & SERVICES","Score":null,"Total":0}
When policy meets reality: the new 18-hour on-call shift policy and the Israeli anesthesia workforce crisis.
Background: The Israeli physician workforce faces multiple challenges. These include planned policies reducing physician on-call from 26 to 18 h and, from 2026, allowing only graduates of Ministry of Health approved foreign medical schools to take the Israeli licensing examination and an ongoing physician shortage (2019: Israel had 3.19 physicians/1000 persons vs. OECD average of 3.49 physicians/1000 persons). This study examines the potential impact of these planned policies on the Israeli anesthesiology workforce.
Methods: Surveys conducted among 34 public and private Israeli hospital anesthesiology department chairs collected data on their department's number of weekday on-call anesthesiologists and current shortage of anesthesiologists. A subsequent survey collected data on each anesthesiologist in the workforce, including the country where they studied medicine.
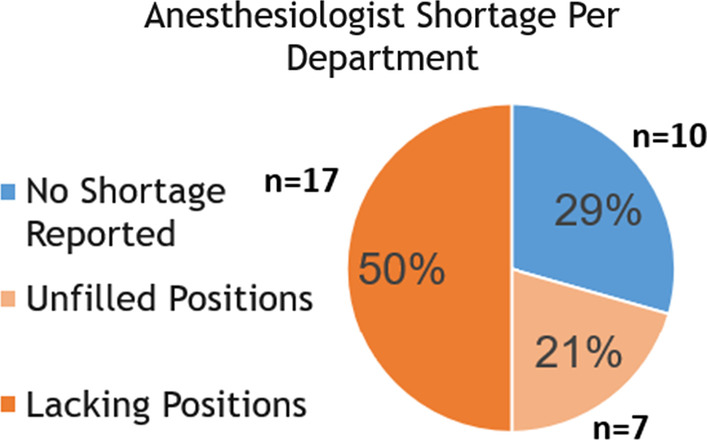
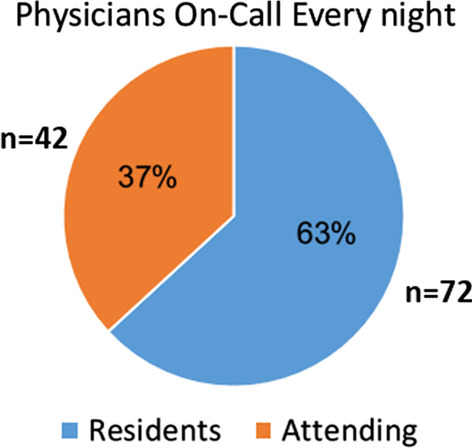
Results: Each weekday night there were 114 on-call anesthesiologists; 72 residents and 42 attendings. Using productive work coefficients, this translates to 104 resident and 51 attending anesthesiologists. Furthermore, 21 departments had existing anesthesia workforce shortages totaling 110 anesthesiologists. There were 873 anesthesiologists from non-OECD countries whose medical schools are not accredited by the World Federation for Medical Education, of whom 332 were residents (61.9% of residents). Only 20.1% of anesthesiology residents were Israeli medical school graduates.
Conclusions: Descriptive survey data assessed the immediate and long-term consequences for the healthcare system and anesthesiology workforce of two new Health Ministry policies. Implementing the 18-h policy will immediately remove from the daytime workforce 155 anesthesiologists and who will be unavailable to staff elective surgery operating rooms. This will compound the current national shortage of 110 anesthesiologists. It is unclear how to replace this shortfall since there are no surplus Israeli physicians and very few Israeli graduates choose anesthesiology as a specialty. This situation will be exacerbated after 2026 when graduates of certain foreign medical schools will be unable to enter the medical workforce, further reducing the pool of potential anesthesiology residents. Both policies were promulgated without adequate operational and budgetary planning or fiscal or workforce resources; implementation of the 18-h on-call policy has already been postponed. Therefore, new or updated policies must be accompanied by specific operational plans, budgetary allocations and funds for additional workforce.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


