Elizabeth L. Norton MD, MS , Linda Farhat MS , Xiaoting Wu PhD , Karen M. Kim MD , Shinichi Fukuhara MD , Himanshu J. Patel MD , George Michael Deeb MD , Bo Yang MD, PhD
{"title":"急性A型主动脉夹层修复的专业化:结果和挑战","authors":"Elizabeth L. Norton MD, MS , Linda Farhat MS , Xiaoting Wu PhD , Karen M. Kim MD , Shinichi Fukuhara MD , Himanshu J. Patel MD , George Michael Deeb MD , Bo Yang MD, PhD","doi":"10.1053/j.semtcvs.2022.05.005","DOIUrl":null,"url":null,"abstract":"<div><p><span>With increasing specialization within the field of cardiac surgery and a positive relationship between case volume and surgical outcomes in many areas, the concept of dedicated aortic surgeons performing acute type A aortic dissection<span> (ATAAD) repair was investigated. From 1996 to 2014, 436 patients underwent open surgical repair of an ATAAD and were subsequently divided based on surgeon subspecialization, aortic-surgeon (AS, n = 401) vs non-aortic-surgeon (NAS, n = 35). Each aortic surgeon performed an average of 13 ATAAD repair operations per year. Preoperative comorbidities were similar between groups. Intraoperatively, the AS group had 36% aortic root replacement vs 23% in the NAS group, </span></span><em>P</em> = 0.12, and 36% zone 1/2/3 arch replacement vs 26% in the NAS group, <em>P</em><span> = 0.20). Postoperatively, the AS group had significantly better outcomes, including intraoperative mortality (1.2% vs 5.7%), 30-day mortality (6.5% vs 17%), and composite outcomes (23% vs 46%). Multivariable logistic regression showed NAS was a risk factor for 30-day mortality with an odds ratio (OR) of 4.4 (</span><em>P</em> = 0.03), as were COPD (OR = 4.0, <em>P</em><span> = 0.046) and cardiogenic shock (OR = 13.4, </span><em>P</em> < 0.0001). The 10-year survival was 66% in the AS group vs 46% in the NAS group, <em>P</em><span> = 0.02. NAS (HR = 2.2), Age (hazard ratio (HR) = 1.05), COPD (HR = 1.96), acute stroke (HR = 3.0), and New York Heart Association class III or IV (HR = 1.75) were significant risk factors for long-term mortality. Managing ATAAD by subspecialized aortic surgeons resulted in improved short- and long-term outcomes. Our specialty could consider ATAAD repair by high-volume aortic surgeons for better patient outcomes.</span></p></div>","PeriodicalId":48592,"journal":{"name":"Seminars in Thoracic and Cardiovascular Surgery","volume":"35 3","pages":"Pages 466-475"},"PeriodicalIF":2.5000,"publicationDate":"2023-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Specialization in Acute Type A Aortic Dissection Repair: The Outcomes and Challenges\",\"authors\":\"Elizabeth L. Norton MD, MS , Linda Farhat MS , Xiaoting Wu PhD , Karen M. Kim MD , Shinichi Fukuhara MD , Himanshu J. Patel MD , George Michael Deeb MD , Bo Yang MD, PhD\",\"doi\":\"10.1053/j.semtcvs.2022.05.005\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><p><span>With increasing specialization within the field of cardiac surgery and a positive relationship between case volume and surgical outcomes in many areas, the concept of dedicated aortic surgeons performing acute type A aortic dissection<span> (ATAAD) repair was investigated. From 1996 to 2014, 436 patients underwent open surgical repair of an ATAAD and were subsequently divided based on surgeon subspecialization, aortic-surgeon (AS, n = 401) vs non-aortic-surgeon (NAS, n = 35). Each aortic surgeon performed an average of 13 ATAAD repair operations per year. Preoperative comorbidities were similar between groups. Intraoperatively, the AS group had 36% aortic root replacement vs 23% in the NAS group, </span></span><em>P</em> = 0.12, and 36% zone 1/2/3 arch replacement vs 26% in the NAS group, <em>P</em><span> = 0.20). Postoperatively, the AS group had significantly better outcomes, including intraoperative mortality (1.2% vs 5.7%), 30-day mortality (6.5% vs 17%), and composite outcomes (23% vs 46%). Multivariable logistic regression showed NAS was a risk factor for 30-day mortality with an odds ratio (OR) of 4.4 (</span><em>P</em> = 0.03), as were COPD (OR = 4.0, <em>P</em><span> = 0.046) and cardiogenic shock (OR = 13.4, </span><em>P</em> < 0.0001). The 10-year survival was 66% in the AS group vs 46% in the NAS group, <em>P</em><span> = 0.02. NAS (HR = 2.2), Age (hazard ratio (HR) = 1.05), COPD (HR = 1.96), acute stroke (HR = 3.0), and New York Heart Association class III or IV (HR = 1.75) were significant risk factors for long-term mortality. Managing ATAAD by subspecialized aortic surgeons resulted in improved short- and long-term outcomes. Our specialty could consider ATAAD repair by high-volume aortic surgeons for better patient outcomes.</span></p></div>\",\"PeriodicalId\":48592,\"journal\":{\"name\":\"Seminars in Thoracic and Cardiovascular Surgery\",\"volume\":\"35 3\",\"pages\":\"Pages 466-475\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2023-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Seminars in Thoracic and Cardiovascular Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S1043067922001241\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Seminars in Thoracic and Cardiovascular Surgery","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S1043067922001241","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
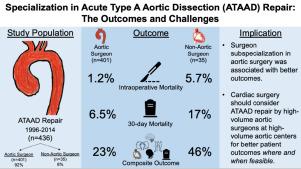
Specialization in Acute Type A Aortic Dissection Repair: The Outcomes and Challenges
With increasing specialization within the field of cardiac surgery and a positive relationship between case volume and surgical outcomes in many areas, the concept of dedicated aortic surgeons performing acute type A aortic dissection (ATAAD) repair was investigated. From 1996 to 2014, 436 patients underwent open surgical repair of an ATAAD and were subsequently divided based on surgeon subspecialization, aortic-surgeon (AS, n = 401) vs non-aortic-surgeon (NAS, n = 35). Each aortic surgeon performed an average of 13 ATAAD repair operations per year. Preoperative comorbidities were similar between groups. Intraoperatively, the AS group had 36% aortic root replacement vs 23% in the NAS group, P = 0.12, and 36% zone 1/2/3 arch replacement vs 26% in the NAS group, P = 0.20). Postoperatively, the AS group had significantly better outcomes, including intraoperative mortality (1.2% vs 5.7%), 30-day mortality (6.5% vs 17%), and composite outcomes (23% vs 46%). Multivariable logistic regression showed NAS was a risk factor for 30-day mortality with an odds ratio (OR) of 4.4 (P = 0.03), as were COPD (OR = 4.0, P = 0.046) and cardiogenic shock (OR = 13.4, P < 0.0001). The 10-year survival was 66% in the AS group vs 46% in the NAS group, P = 0.02. NAS (HR = 2.2), Age (hazard ratio (HR) = 1.05), COPD (HR = 1.96), acute stroke (HR = 3.0), and New York Heart Association class III or IV (HR = 1.75) were significant risk factors for long-term mortality. Managing ATAAD by subspecialized aortic surgeons resulted in improved short- and long-term outcomes. Our specialty could consider ATAAD repair by high-volume aortic surgeons for better patient outcomes.
期刊介绍:
Seminars in Thoracic and Cardiovascular Surgery is devoted to providing a forum for cardiothoracic surgeons to disseminate and discuss important new information and to gain insight into unresolved areas of question in the specialty. Each issue presents readers with a selection of original peer-reviewed articles accompanied by editorial commentary from specialists in the field. In addition, readers are offered valuable invited articles: State of Views editorials and Current Readings highlighting the latest contributions on central or controversial issues. Another prized feature is expert roundtable discussions in which experts debate critical questions for cardiothoracic treatment and care. Seminars is an invitation-only publication that receives original submissions transferred ONLY from its sister publication, The Journal of Thoracic and Cardiovascular Surgery. As we continue to expand the reach of the Journal, we will explore the possibility of accepting unsolicited manuscripts in the future.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


